
Step In, Step Out from the First Lockdown: An Exploration of COVID-19 Perceptions in France and Quebec

 , , and
, , and
Abstract
:1. Introduction
1.1. Perception of Risk in the Pandemic Context
1.2. The Present Study
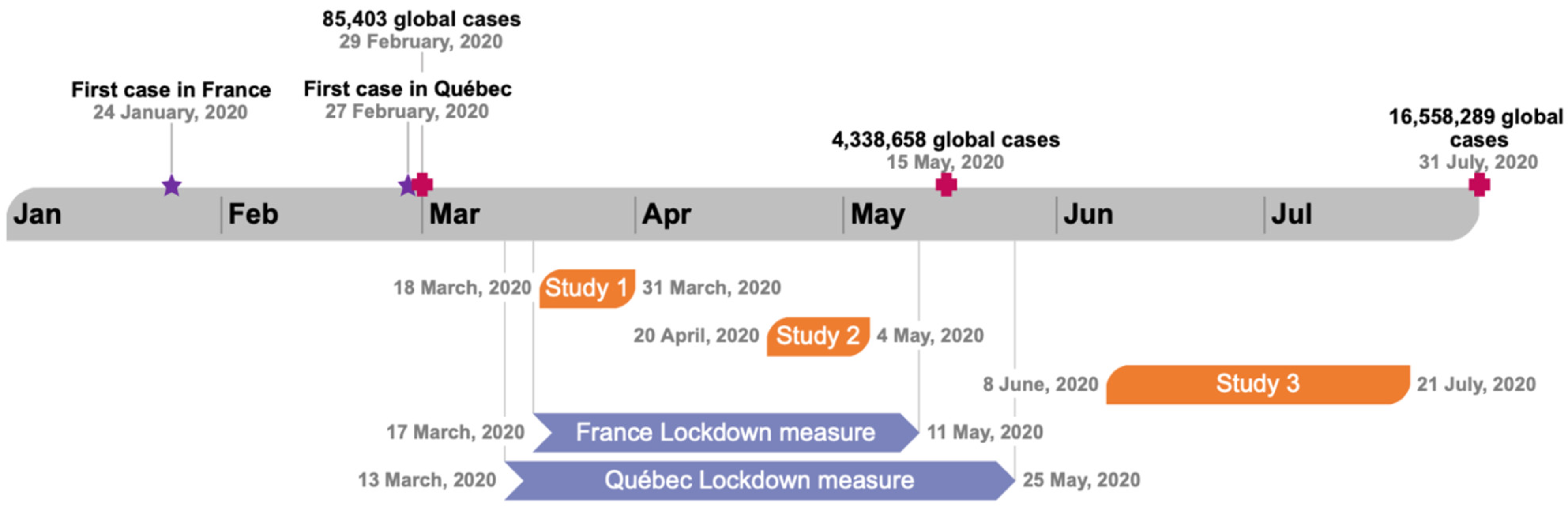
2. Study 1, COVID-19 Perceptions at the Beginning of Lockdown
2.1. Methods
2.1.1. Procedure
2.1.2. Participants
2.1.3. Measures
2.1.4. Data Analysis
2.2. Results
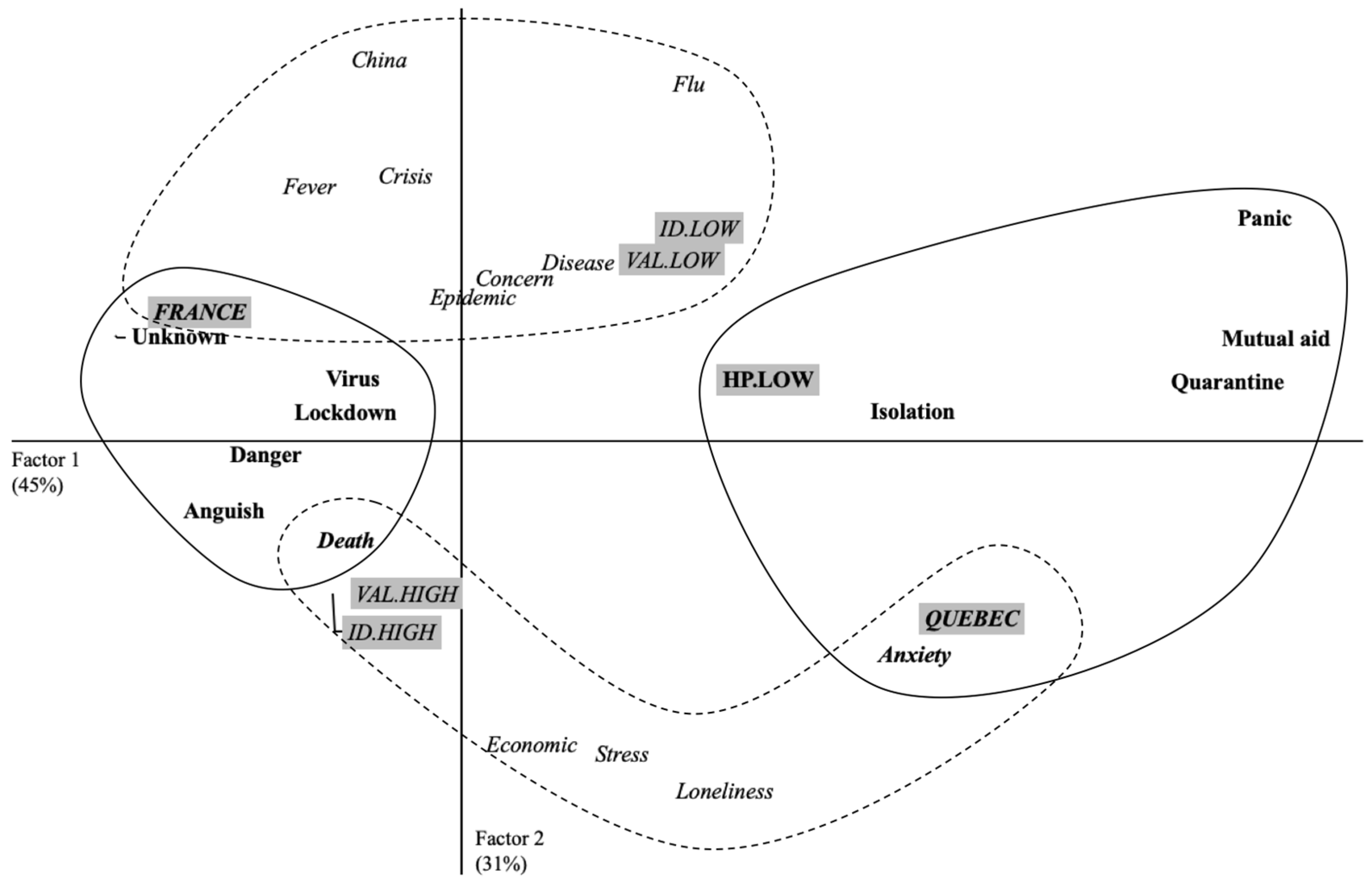
2.2.1. Perceptions of COVID-19 at the Beginning of Lockdown
2.2.2. Personal Involvement and Health Practices
3. Study 2, COVID-19 Perceptions during the Lockdown
3.1. Method
3.1.1. Procedure
3.1.2. Participants
3.1.3. Measures
3.2. Results
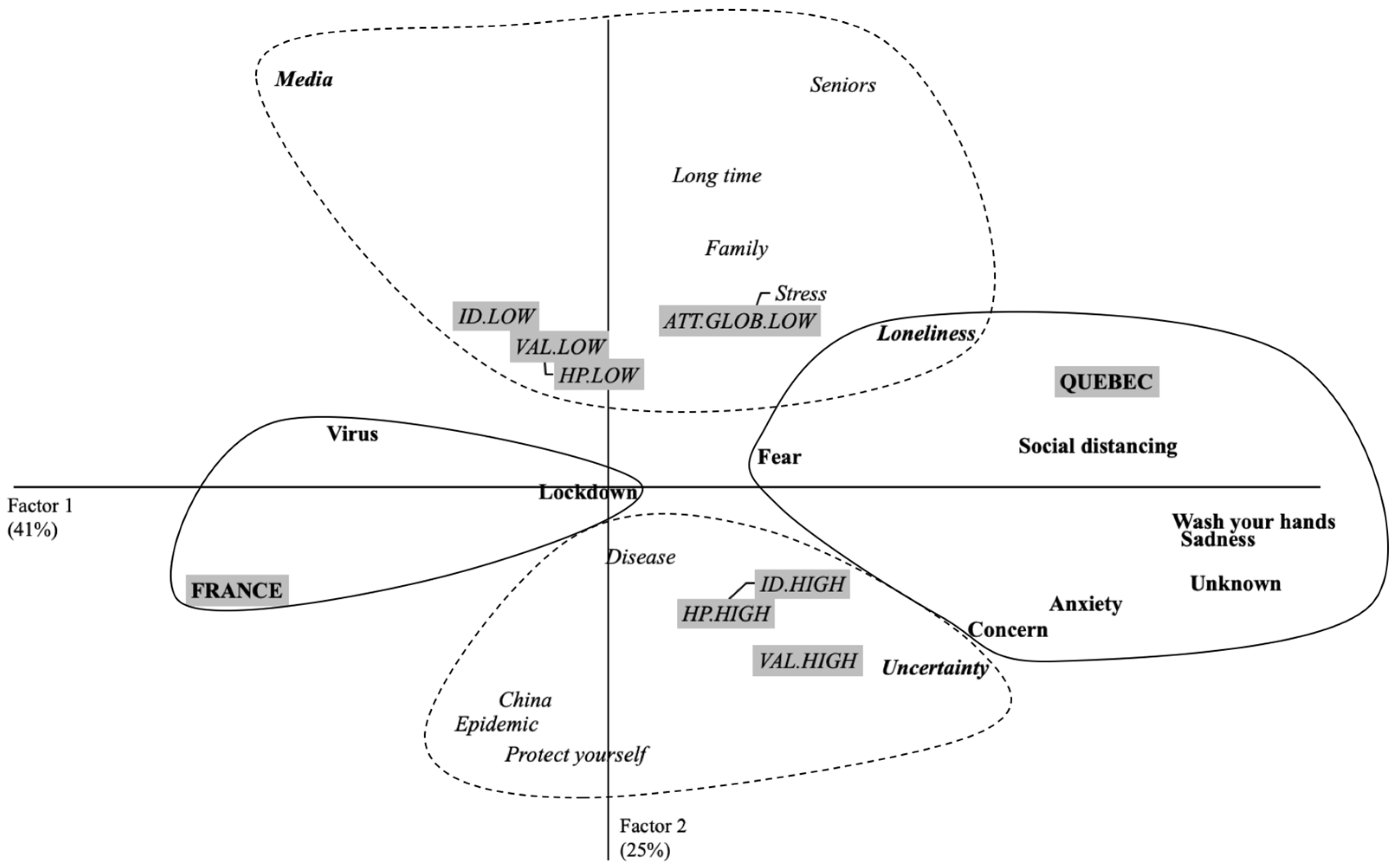
3.2.1. Perceptions of COVID-19, 1 Month after the Beginning of Lockdown
3.2.2. Personal Involvement, Health Practices and Attitudes toward Lockdown Measures
4. Study 3, COVID-19 Perceptions at the Lockdown Exit
4.1. Method
4.1.1. Procedure
4.1.2. Participants
4.1.3. Measures
4.2. Results
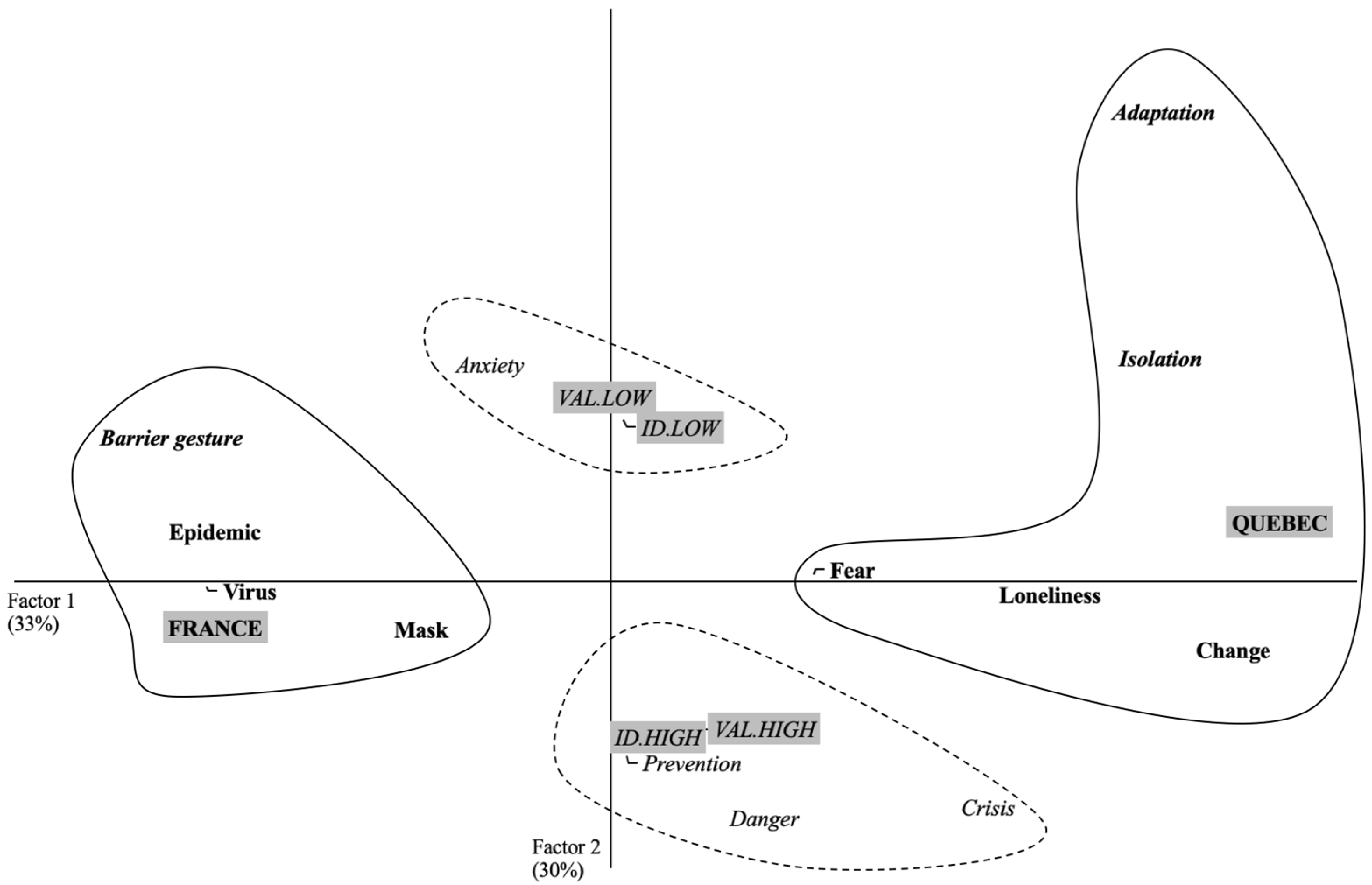
4.2.1. Perceptions of COVID-19 at the Lockdown Exit
4.2.2. Personal Involvement, Health Practices, and Attitudes toward Lockdown Exit Measures
5. General Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fang, Y.; Nie, Y.; Penny, M. Transmission dynamics of the COVID-19 outbreak and effectiveness of government interventions: A data-driven analysis. J. Med. Virol. 2020, 92, 645–659. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y.; Liu, X.; Chen, R.; Tang, C.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A Nationwide Analysis. Respir. Med. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, N. Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus and COVID-19 pandemic: A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Bruns, D.P.; Kraguljac, N.V.; Bruns, T.R. COVID-19: Facts, Cultural Considerations, and Risk of Stigmatization. J. Transcult. Nurs. 2020, 31, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Zambrano-Monserrate, M.A.; Ruano, M.A.; Sanchez-Alcalde, L. Indirect effects of COVID-19 on the environment. Sci. Total. Environ. 2020, 728, 138813. [Google Scholar] [CrossRef] [PubMed]
- Bol, D.; Giani, M.; Blais, A.; Loewen, P.J. The effect of COVID-19 lockdowns on political support: Some good news for democracy? Eur. J. Politi-Res. 2020, 60, 497–505. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- McKibbin, W.; Fernando, R. The Global Macroeconomic Impacts of COVID-19: Seven Scenarios. Asian Econ. Pap. 2021, 20, 1–30. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Bonetto, E.; Delouvée, S.; Mahfud, Y.; Adam-Troian, J. National Identification, a Social Cure for COVID-19? Evidence from 67 Countries. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Atalan, A. Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and economy-perspective. Ann. Med. Surg. 2020, 56, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Cerbara, L.; Ciancimino, G.; Crescimbene, M.; La Longa, F.; Parsi, M.R.; Tintori, A.; Palomba, R. A nation-wide survey on emotional and psychological impacts of COVID-19 social distancing. Eur. Rev. Med Pharmacol. Sci. 2020, 24, 7155–7163. [Google Scholar] [PubMed]
- Pennycook, G.; McPhetres, J.; Zhang, Y.; Lu, J.G.; Rand, D.G. Fighting COVID-19 Misinformation on Social Media: Experimental Evidence for a Scalable Accuracy-Nudge Intervention. Psychol. Sci. 2020, 31, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Gonsalves, G.; Staley, P. Panic, Paranoia, and Public Health—The AIDS Epidemic’s Lessons for Ebola. N. Engl. J. Med. 2014, 371, 2348–2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.-J.; Huang, N.; Lee, C.-H.; Hsu, Y.-J.; Hsieh, C.-J.; Chou, Y.-J. The Impact of the SARS Epidemic on the Utilization of Medical Services: SARS and the Fear of SARS. Am. J. Public Heal. 2004, 94, 562–564. [Google Scholar] [CrossRef]
- Emobbs, D.; Hagan, C.; Dalgleish, T.; Esilston, B.; Prévost, C. The ecology of human fear: Survival optimization and the nervous system. Front. Neurosci. 2015, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Jaspal, R.; Nerlich, B. Social representations, identity threat, and coping amid COVID-19. Psychol. Trauma Theory Res. Prac. Policy 2020, 12, S249–S251. [Google Scholar] [CrossRef]
- Idoiaga Mondragon, N.; Gil de Montes, L.; Valencia, J. Understanding an Ebola outbreak: Social representations of emerging infectious diseases. J. Health Psychol. 2017, 22, 951–960. [Google Scholar] [CrossRef]
- Slovic, P. Trust, Emotion, Sex, Politics, and Science: Surveying the Risk-Assessment Battlefield. Risk Anal. 1999, 19, 689–701. [Google Scholar] [CrossRef] [Green Version]
- Joffe, H. Risk: From perception to social representation. Br. J. Soc. Psychol. 2003, 42, 55–73. [Google Scholar] [CrossRef]
- Apostolidis, T.; Dany, L. Pensée sociale et risques dans le domaine de la santé: Le regard des représentations sociales. Psychol. Française 2012, 57, 67–81. [Google Scholar] [CrossRef]
- Gilbert, C. La fabrique des risques. Cah. Int. Sociol. 2003, 114, 55–72. [Google Scholar] [CrossRef]
- Rudnick, A. Social, Psychological, and Philosophical Reflections on Pandemics and Beyond. Societies 2020, 10, 42. [Google Scholar] [CrossRef]
- DAS, T.; Teng, B.-S. Strategic risk behaviour and its temporalities: Between risk propensity and decision context. J. Manag. Stud. 2001, 38, 515–534. [Google Scholar] [CrossRef]
- Washer, P. Representations of SARS in the British newspapers. Soc. Sci. Med. 2004, 59, 2561–2571. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Schaller, M.; Murray, D.R.; Bangerter, A. Implications of the behavioural immune system for social behaviour and human health in the modern world. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140105. [Google Scholar] [CrossRef]
- Chen, S.; Bonanno, G.A. Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychol. Trauma Theory Res. Prac. Policy 2020, 12, S51–S54. [Google Scholar] [CrossRef] [PubMed]
- Luchetti, M.; Lee, J.H.; Aschwanden, D.; Sesker, A.; Strickhouser, J.E.; Terracciano, A.; Sutin, A.R. The trajectory of loneliness in response to COVID-19. Am. Psychol. 2020, 75, 897–908. [Google Scholar] [CrossRef]
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Khubchandani, J. Knowledge, Attitude, Perceptions and Practice towards COVID-19: A Systematic Review and Meta-Analysis. Infect. Dis. 2020. Available online: 10.1101/2020.06.24.20138891.
- France-Canada-Québec. 400 ans de Relations D’exception: 400 ans de Relations D’exception; Presses de l’Université de Montréal: Montreal, QC, Canada, 2008; Available online: https://www.jstor.org/stable/j.ctv69t8nd (accessed on 16 October 2020).
- Herzlich, C.; Adam, P. Sociologie de la Maladie et de la Médecine; Nathan: Paris, France, 1994. [Google Scholar]
- Guan, Y.; Deng, H.; Zhou, X. Understanding the impact of the COVID-19 pandemic on career development: Insights from cultural psychology. J. Vocat. Behav. 2020, 119, 103438. [Google Scholar] [CrossRef] [PubMed]
- Barhoumi, M.; Jonchery, A.; Lombardo, P.; Le Minez, S.; Mainaud, T.; Raynaud, E.; Pailhé, A.; Solaz, A.; Pollak, C. Les inégalités sociales à l’épreuve de la crise sanitaire: Un bilan du premier confinement. In France, Portrait Social; Institut National de la Statistique et des Études Économiques (INSEE): Paris, France, 2020; pp. 11–44. Available online: https://hal.archives-ouvertes.fr/hal-03045998 (accessed on 18 October 2021).
- Lo Monaco, G.; Piermattéo, A.; Rateau, P.; Tavani, J.L. Methods for Studying the Structure of Social Representations: A Critical Review and Agenda for Future Research: Methods and Structure of Social Representations. J. Theory Soc. Behav. 2017, 47, 306–331. [Google Scholar] [CrossRef] [Green Version]
- Ernst-Vintila, A.; Delouvée, S.; Roland-Lévy, C. Under threat. Lay thinking about terrorism and the three-dimensional model of personal involvement: A social psychological analysis. J. Risk Res. 2011, 14, 297–324. [Google Scholar] [CrossRef]
- Demarque, C.; Monaco, G.L.; Apostolidis, T.; Guimelli, C. Socialisation, perspectives temporelles et implication personnelle: Une étude dans le champ de l’environnement. Les Cah. Int. Psychol. Soc. 2012, 92, 351–369. [Google Scholar] [CrossRef] [Green Version]
- Deschamps, J.C. Analyse des correspondances et variations des contenus de représentations sociales. In Méthodes D’étude des Représentations Sociales; Abric, C., Ed.; Erès: Ramonville Saint-Agnes, France, 2003; pp. 179–199. [Google Scholar] [CrossRef]
- Maio, G.R.; Haddock, G. The Psychology of Attitudes and Attitude Change; SAGE: Los Angeles, CA, USA; London, UK, 2009; 276p. [Google Scholar]
- Brock, T.C.; Green, M.C. Persuasion: Psychological Insights and Perspectives; SAGE: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Rev. Bras. Psiquiatr. 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Pakpour, A.H.; Griffiths, M.D. The fear of COVID-19 and its role in preventive behaviors. J. Concurr. Disord. 2020. Available online: https://concurrentdisorders.ca/2020/04/03/the-fear-of-covid-19-and-its-role-in-preventive-behaviors (accessed on 26 October 2021).
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as Analysis and Risk as Feelings: Some Thoughts about Affect, Reason, Risk, and Rationality. Risk Anal. 2004, 24, 311–322. [Google Scholar] [CrossRef]
- Wardman, J. Sociocultural vectors of effective risk communication. J. Risk Res. 2014, 17, 1251–1257. [Google Scholar] [CrossRef]
- Engdahl, E.; Lidskog, R. Risk, communication and trust: Towards an emotional understanding of trust. Public Underst. Sci. 2012, 23, 703–717. [Google Scholar] [CrossRef] [PubMed]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Papageorge, N.W.; Zahn, M.V.; Belot, M.; Broek-Altenburg, E.V.D.; Choi, S.; Jamison, J.C.; Tripodi, E. Socio-demographic factors associated with self-protecting behavior during the Covid-19 pandemic. J. Popul. Econ. 2021, 34, 691–738. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 255) | France (n = 146) | Quebec (n = 109) |
|---|---|---|---|
| Age in year | 37 ± 12.8 | 36.1 ± 12.8 | 38.2 ± 12.7 |
| Gender | |||
| Men | 49 | 27 | 22 |
| Women | 203 | 117 | 86 |
| Other | 3 | 2 | 1 |
| Social professional category | |||
| Managers and senior professionals | 73 | 46 | 27 |
| Employees | 63 | 37 | 26 |
| Students | 45 | 33 | 12 |
| Intermediate Professions | 21 | 7 | 14 |
| Persons without professional activity | 9 | 6 | 3 |
| Retired | 17 | 7 | 10 |
| Liberal Professions | 3 | 3 | 0 |
| Workers | 4 | 3 | 1 |
| Farmers | 1 | 1 | 0 |
| Other | 19 | 3 | 16 |
| Identification with COVID-19 | 4.50 ± 0.68 | 4.41 ± 0.75 | 4.61 ± 0.56 |
| Valuation of the COVID-19 | 4.58 ± 0.51 | 4.50 ± 0.58 | 4.67 ± 0.38 |
| Perceived capacity for action | 3.61 ± 0.78 | 3.36 ± 0.70 | 3.94 ± 0.76 |
| Health practices | 4.15 ± 0.45 | 4.15 ± 0.48 | 4.15 ± 0.40 |
| Variables | Overall (n = 230) | France (n = 119) | Quebec (n = 111) |
|---|---|---|---|
| Age in year | 36.5 ± 13.6 | 31.7 ± 12.2 | 41.6 ± 13.1 |
| Gender | |||
| Men | 55 | 34 | 21 |
| Women | 172 | 84 | 88 |
| Other | 3 | 1 | 2 |
| Social professional category | |||
| Managers and senior professionals | 75 | 39 | 36 |
| Employees | 52 | 24 | 28 |
| Students | 51 | 36 | 15 |
| Intermediate Professions | 18 | 6 | 12 |
| Persons without professional activity | 8 | 7 | 1 |
| Retired | 14 | 3 | 11 |
| Liberal Professions | 5 | 1 | 4 |
| Workers | 1 | 1 | 0 |
| Farmers | 2 | 2 | 0 |
| Other | 4 | 0 | 4 |
| Identification with COVID-19 | 4.33 ± 0.71 | 4.24 ± 0.74 | 4.43 ± 0.67 |
| Valuation of the COVID-19 | 4.45 ± 0.57 | 4.37 ± 0.59 | 4.53 ± 0.52 |
| Perceived capacity for action | 3.52 ± 0.81 | 3.30 ± 0.80 | 3.76 ± 0.75 |
| Health practices | 4.12 ± 0.48 | 4.08 ± 0.46 | 4.16 ± 0.50 |
| Attitudes toward lockdown measures | 4.22 ± 0.93 | 4.10 ± 0.98 | 4.35 ± 0.87 |
| Variables | Overall (n = 143) | France (n = 72) | Quebec (n = 71) |
|---|---|---|---|
| Age in year | 35.9 ± 12.8 | 31.8 ± 10.6 | 40.1 ± 13.5 |
| Gender | |||
| Men | 33 | 16 | 17 |
| Women | 108 | 55 | 53 |
| Other | 2 | 1 | 1 |
| Social professional category | |||
| Managers and senior professionals | 45 | 25 | 20 |
| Employees | 28 | 15 | 13 |
| Students | 30 | 19 | 11 |
| Intermediate Professions | 8 | 5 | 3 |
| Persons without professional activity | 8 | 2 | 6 |
| Retired | 10 | 2 | 8 |
| Liberal Professions | 12 | 2 | 10 |
| Workers | 0 | 0 | 0 |
| Farmers | 1 | 1 | 0 |
| Other | 1 | 1 | 0 |
| Identification with COVID-19 | 4.18 ± 0.85 | 4.15 ± 0.85 | 4.21 ± 0.85 |
| Valuation of the COVID-19 | 4.26 ± 0.76 | 4.21 ± 0.76 | 4.31 ± 0.77 |
| Perceived capacity for action | 3.51 ± 0.79 | 3.39 ± 0.80 | 3.63 ± 0.78 |
| Health practices | 3.90 ± 0.62 | 3.76 ± 0.62 | 4.04 ± 0.59 |
| Attitudes toward lockdown measures | 3.67 ± 0.91 | 3.72 ± 0.88 | 3.63 ± 0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
David, J.-C.; Nadarajah, K.; Niang, A.; Delouvée, S.; Goyette, M.; Bordel, S.; Somat, A. Step In, Step Out from the First Lockdown: An Exploration of COVID-19 Perceptions in France and Quebec. Infect. Dis. Rep. 2021, 13, 965-977. https://doi.org/10.3390/idr13040089
David J-C, Nadarajah K, Niang A, Delouvée S, Goyette M, Bordel S, Somat A. Step In, Step Out from the First Lockdown: An Exploration of COVID-19 Perceptions in France and Quebec. Infectious Disease Reports. 2021; 13(4):965-977. https://doi.org/10.3390/idr13040089
Chicago/Turabian StyleDavid, Jean-Charles, Kévin Nadarajah, Anta Niang, Sylvain Delouvée, Martin Goyette, Stéphanie Bordel, and Alain Somat. 2021. "Step In, Step Out from the First Lockdown: An Exploration of COVID-19 Perceptions in France and Quebec" Infectious Disease Reports 13, no. 4: 965-977. https://doi.org/10.3390/idr13040089