
Age at Natural Menopause in Women Living with HIV: A Cross-Sectional Study Comparing Self-Reported and Biochemical Data
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
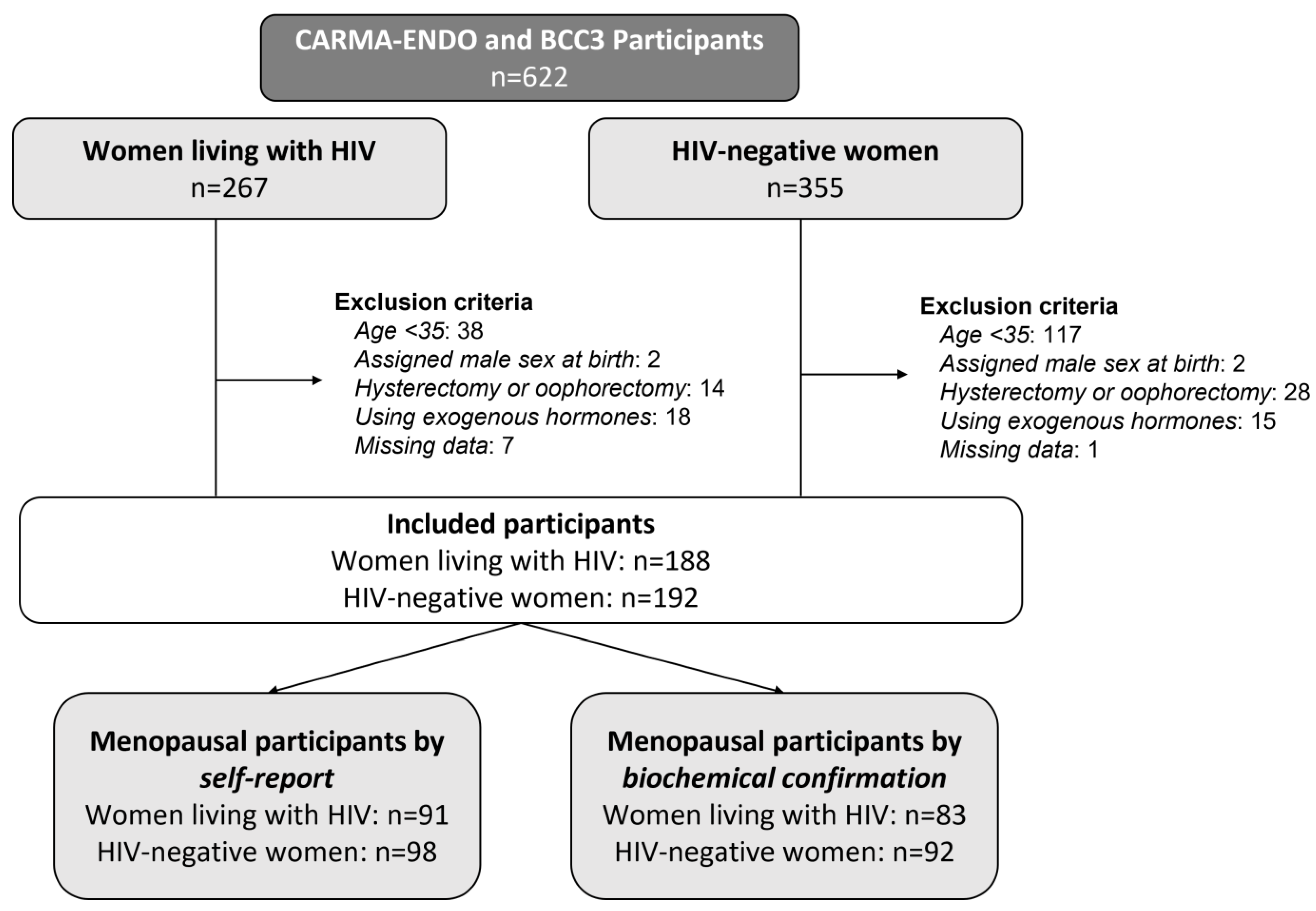
2.1. Study Design and Participants
2.2. Procedures
2.3. Variables
2.4. Defining Menopause Status and Age at Menopause
2.5. Sample Size and Statistical Analysis
3. Results
3.1. Participant Demographics
3.2. Classification of Reproductive Phase
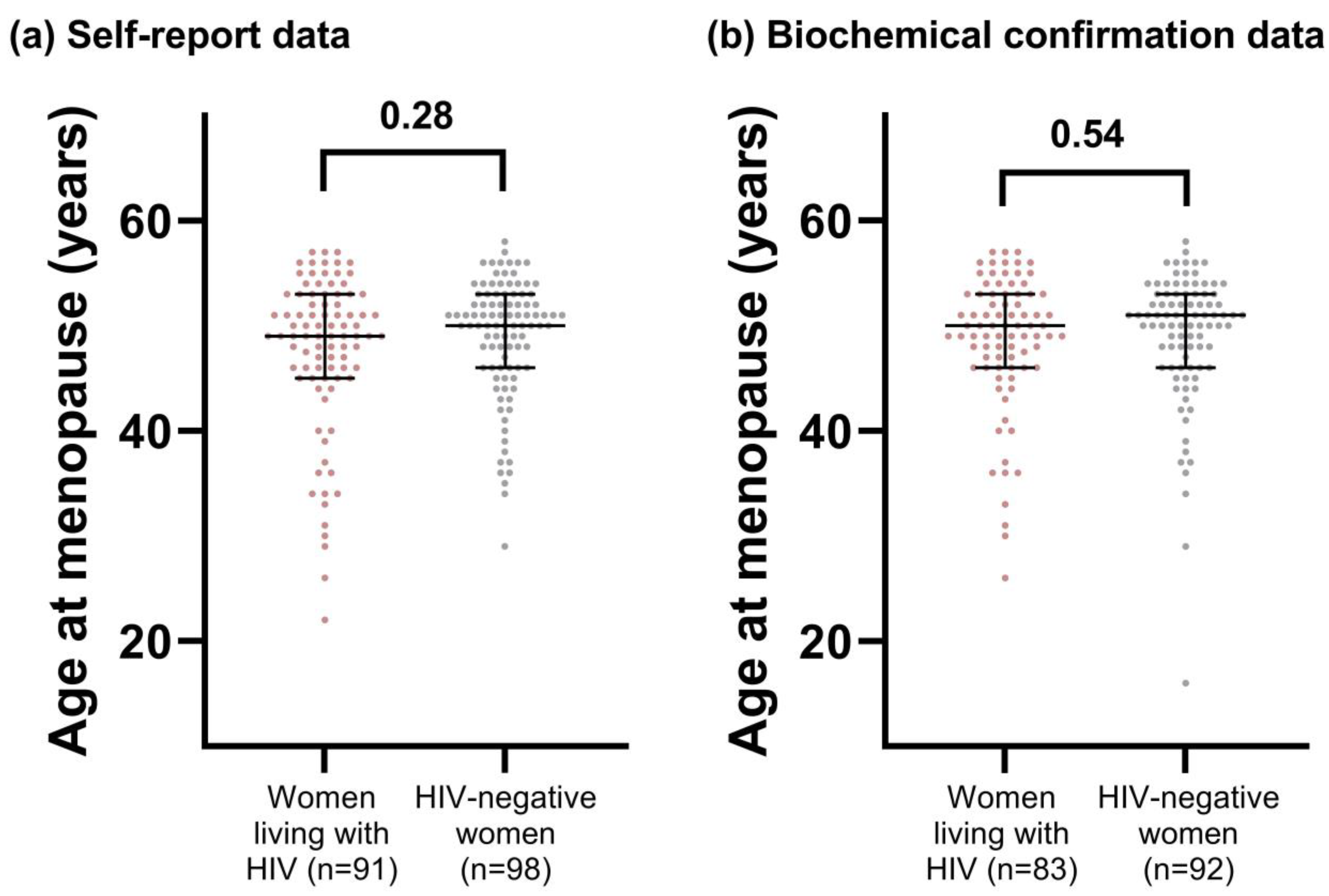
3.3. Age at Menopause
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global HIV & AIDS Statistics—Fact Sheet | UNAIDS. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 29 November 2022).
- Smit, M.; Brinkman, K.; Geerlings, S.; Smit, C.; Thyagarajan, K.; van Sighem, A.V.; de Wolf, F.; Hallett, T.B. Future Challenges for Clinical Care of an Ageing Population Infected with HIV: A Modelling Study. Lancet Infect. Dis. 2015, 15, 818. [Google Scholar] [CrossRef] [PubMed]
- Peacock, K.; Ketvertis, K.M. Menopause; StatPearls: Treaure Island, FL, USA, 2021. [Google Scholar]
- El Khoudary, S.R.; Greendale, G.; Crawford, S.L.; Avis, N.E.; Brooks, M.M.; Thurston, R.C.; Karvonen-Gutierrez, C.; Waetjen, L.E.; Matthews, K. The Menopause Transition and Women’s Health at Midlife: A Progress Report from the Study of Women’s Health Across the Nation (SWAN). Menopause 2019, 26, 1227. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Goldgar, D.; Moy, A. Total Bone Calcium in Normal Women: Effect of Age and Menopause Status. J. Bone Miner. Res. 1987, 2, 491–496. [Google Scholar] [CrossRef]
- Menopause. Available online: https://www.who.int/news-room/fact-sheets/detail/menopause (accessed on 21 February 2023).
- Boonyanurak, P.; Bunupuradah, T.; Wilawan, K.; Lueanyod, A.; Thongpaeng, P.; Chatvong, D.; Sophonphan, J.; Saeloo, S.; Ananworanich, J.; Chaithongwongwatthana, S. Age at Menopause and Menopause-Related Symptoms in Human Immunodeficiency Virus-Infected Thai Women. Menopause 2012, 19, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Calvet, G.A.; Grinsztejn, B.G.J.; Quintana, M.D.S.B.; Derrico, M.; Jalil, E.M.; Cytryn, A.; de Andrade, A.C.V.; Moreira, R.I.; Alves, M.R.; Dos Santos, V.G.V.; et al. Predictors of Early Menopause in HIV-Infected Women: A Prospective Cohort Study. Am. J. Obstet. Gynecol. 2015, 212, 765.e1–765.e13. [Google Scholar] [CrossRef]
- Ferreira, C.E.; Pinto-Neto, A.M.; Conde, D.M.; Costa-Paiva, L.; Morais, S.S.; Magalhães, J. Menopause Symptoms in Women Infected with HIV: Prevalence and Associated Factors. Gynecol. Endocrinol. 2007, 23, 198–205. [Google Scholar] [CrossRef]
- Andany, N.; Kaida, A.; de Pokomandy, A.; Yudin, M.H.; Wang, L.; Kennedy, V.L.; Webster, K.; Loutfy, M.; CHIWOS Research Team. Prevalence and Correlates of Early-Onset Menopause among Women Living with HIV in Canada. Menopause 2020, 27, 66–75. [Google Scholar] [CrossRef]
- Schoenbaum, E.E.; Hartel, D.; Lo, Y.; Howard, A.A.; Floris-Moore, M.; Arnsten, J.H.; Santoro, N. HIV Infection, Drug Use, and Onset of Natural Menopause. Clin. Infect. Dis. 2005, 41, 1517–1524. [Google Scholar] [CrossRef]
- De Pommerol, M.; Hessamfar, M.; Lawson-Ayayi, S.; Neau, D.; Geffard, S.; Farbos, S.; Uwamaliya, B.; Vandenhende, M.A.; Pellegrin, J.L.; Blancpain, S.; et al. Menopause and HIV Infection: Age at Onset and Associated Factors, ANRS CO3 Aquitaine Cohort. Int. J. STD AIDS 2011, 22, 67–72. [Google Scholar] [CrossRef]
- Fantry, L.E.; Zhan, M.; Taylor, G.H.; Sill, A.M.; Flaws, J.A. Age of Menopause and Menopausal Symptoms in HIV-Infected Women. AIDS Patient Care STDs 2005, 19, 703–711. [Google Scholar] [CrossRef]
- Parker, S.E.; Troisi, R.; Wise, L.A.; Palmer, J.R.; Titus-Ernstoff, L.; Strohsnitter, W.C.; Hatch, E.E. Menarche, Menopause, Years of Menstruation, and the Incidence of Osteoporosis: The Influence of Prenatal Exposure to Diethylstilbestrol. J. Clin. Endocrinol. Metab. 2014, 99, 594. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Aggarwal, B.; Beckie, T.M.; Hodis, H.N.; Johnson, A.E.; Langer, R.D.; Limacher, M.C.; Manson, J.E.; Stefanick, M.L.; Allison, M.A.; et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement from the American Heart Association. Circulation 2020, 142, 506–532. [Google Scholar] [CrossRef] [PubMed]
- Shuster, L.T.; Rhodes, D.J.; Gostout, B.S.; Grossardt, B.R.; Rocca, W.A. Premature Menopause or Early Menopause: Long-Term Health Consequences. Maturitas 2010, 65, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Van Ommen, C.E.; Albert, A.Y.; King, E.M.; Murray, M.C.M. Age at Menopause in Women Living with HIV: A Systematic Review. Menopause 2021, 28, 240. [Google Scholar] [CrossRef]
- Prior, J.C. Adaptive, Reversible, Hypothalamic Reproductive Suppression: More than Functional Hypothalamic Amenorrhea. Front. Endocrinol. 2022, 13, 893889. [Google Scholar] [CrossRef]
- King, E.M.; Albert, A.Y.; Murray, M.C.M. HIV and Amenorrhea: A Meta-Analysis. AIDS 2019, 33, 483–491. [Google Scholar] [CrossRef]
- King, E.M.; Nesbitt, A.; Albert, A.Y.K.; Pick, N.; Cote, H.C.F.; Maan, E.J.; Prior, J.C.; Murray, M.C.M. Prolonged Amenorrhea and Low Hip Bone Mineral Density in Women Living with HIV—A Controlled Cross-Sectional Study. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 83, 486–495. [Google Scholar] [CrossRef]
- Fourman, L.T.; Fazeli, P.K. Review: Neuroendocrine Causes of Amenorrhea—An Update. J. Clin. Endocrinol. Metab. 2015, 100, 812. [Google Scholar] [CrossRef]
- Katz, N.; Mazer, N.A. The Impact of Opioids on the Endocrine System. Clin. J. Pain 2009, 25, 170–175. [Google Scholar] [CrossRef]
- Abs, R.; Verhelst, J.; Maeyaert, J.; Van Buyten, J.-P.; Opsomer, F.; Adriaensen, H.; Verlooy, J.; Van Havenbergh, T.; Smet, M.; Van Acker, K. Endocrine Consequences of Long-Term Intrathecal Administration of Opioids. J. Clin. Endocrinol. Metab. 2000, 85, 2215–2222. [Google Scholar] [CrossRef]
- Roberts, R.E.; Farahani, L.; Webber, L.; Jayasena, C. Current Understanding of Hypothalamic Amenorrhoea. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820945854. [Google Scholar] [CrossRef]
- Cejtin, H.E.; Evans, C.T.; Greenblatt, R.; Minkoff, H.; Weber, K.M.; Wright, R.; Colie, C.; Golub, E.; Massad, L.S. Prolonged Amenorrhea and Resumption of Menses in Women with HIV. J. Women’s Health 2018, 27, 1441–1448. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E. Endocrinology of the Menopause. Endocrinol. Metab. Clin. N. Am. 2015, 44, 485. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; Ackerman, K.E.; Berga, S.L.; Kaplan, J.R.; Mastorakos, G.; Misra, M.; Murad, M.H.; Santoro, N.F.; Warren, M.P. Functional Hypothalamic Amenorrhea: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 1413–1439. [Google Scholar] [CrossRef]
- Swann, S.A.; Kaida, A.; Nicholson, V.; Brophy, J.; Campbell, A.R.; Carter, A.; Elwood, C.; Gebremedhen, T.; Gormley, R.; King, E.M.; et al. British Columbia CARMA-CHIWOS Collaboration (BCC3): Protocol for a Community-Collaborative Cohort Study Examining Healthy Ageing with and for Women Living with HIV. BMJ Open 2021, 11, 46558. [Google Scholar] [CrossRef]
- Cejtin, H.E.; Kalinowski, A.; Bacchetti, P.; Taylor, R.N.; Watts, D.H.; Kim, S.; Massad, L.S.; Preston-Martin, S.; Anastos, K.; Moxley, M.; et al. Effects of Human Immunodeficiency Virus on Protracted Amenorrhea and Ovarian Dysfunction. Obstet. Gynecol. 2006, 108, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.W.; Sammel, M.D.; Lin, H.; Gracia, C.R. Obesity and Reproductive Hormone Levels in the Transition to Menopause. Menopause 2010, 17, 726. [Google Scholar] [CrossRef]
- Tao, X.; Jiang, A.; Yin, L.; Li, Y.; Tao, F.; Hu, H. Body Mass Index and Age at Natural Menopause: A Meta-Analysis. Menopause 2015, 22, 469–474. [Google Scholar] [CrossRef]
- Gold, E.B.; Bromberger, J.; Crawford, S.; Samuels, S.; Greendale, G.A.; Harlow, S.D.; Skurnick, J. Factors Associated with Age at Natural Menopause in a Multiethnic Sample of Midlife Women. Am. J. Epidemiol. 2001, 153, 865–874. [Google Scholar] [CrossRef]
- Costanian, C.; McCague, H.; Tamim, H. Age at Natural Menopause and Its Associated Factors in Canada: Cross-Sectional Analyses from the Canadian Longitudinal Study on Aging. Menopause 2018, 25, 265–272. [Google Scholar] [CrossRef]
- Zanni, M.V.; Currier, J.S.; Kantor, A.; Smeaton, L.; Rivard, C.; Taron, J.; Burdo, T.H.; Badal-Faesen, S.; Lalloo, U.G.; Pinto, J.A.; et al. Correlates and Timing of Reproductive Aging Transitions in a Global Cohort of Midlife Women with Human Immunodeficiency Virus: Insights From the REPRIEVE Trial. J. Infect. Dis. 2020, 222, S20–S30. [Google Scholar] [CrossRef] [PubMed]
- King, E.M.; Kaida, A.; Mayer, U.; Albert, A.; Gormley, R.; De Pokomandy, A.; Nicholson, V.; Cardinal, C.; Islam, S.; Loutfy, M.; et al. Brief Report: Undertreated Midlife Symptoms for Women Living with HIV Linked to Lack of Menopause Discussions with Care Providers. J. Acquir. Immune Defic. Syndr. 2022, 89, 505–510. [Google Scholar] [CrossRef]
- Luborsky, J.L.; Meyer, P.; Sowers, M.F.; Gold, E.B.; Santoro, N. Premature Menopause in a Multi-ethnic Population Study of the Menopause Transition*. Hum. Reprod. 2003, 18, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Mishra, G.D.; Pandeya, N.; Dobson, A.J.; Chung, H.-F.; Anderson, D.; Kuh, D.; Sandin, S.; Giles, G.G.; Bruinsma, F.; Hayashi, K.; et al. Early Menarche, Nulliparity and the Risk for Premature and Early Natural Menopause. Hum. Reprod. 2017, 32, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Cramer, D.W.; Barbieri, R.L.; Xu, H.; Reichardt, J.K. Determinants of Basal Follicle-Stimulating Hormone Levels in Premenopausal Women. J. Clin. Endocrinol. Metab. 1994, 79, 1105–1109. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.P.; Siris, E.S.; Petrovich, C. The Influence of Severe Illness on Gonadotropin Secretion in the Postmenopausal Female. J. Clin. Endocrinol. Metab. 1977, 45, 99–104. [Google Scholar] [CrossRef]
- Kestler, M.; Murray, M.; Money, D.; Sauve, L.; Pick, N. The Oak Tree Clinic: The Envisioned Model of Care for Women Living with Human Immunodeficiency Virus in Canada. Women’s Health Issues 2018, 28, 197–198. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Women Living with HIV (n = 188) | HIV-Negative Women (n = 192) | p-Value | |
|---|---|---|---|
| Socio-demographic data | |||
| Age, median [IQR] * years | 49.2 [43.4 to 55.8] | 51.0 [43.8 to 58.1] | 0.16 |
| Ethnicity, n (%) | 0.002 | ||
| White | 75 (39.9) | 79 (41.1) | |
| Indigenous | 66 (35.1) | 54 (28.1) | |
| African, Caribbean, or Black | 26 (13.8) | 13 (6.8) | |
| Other/mixed | 21 (11.2) | 46 (24.0) | |
| Income, n (%) | 0.003 | ||
| <CAD 20,000 †/year | 92 (52.3) | 66 (36.1) | |
| ≥CAD 20,000/year | 86 (46.7) | 117 (63.9) | |
| Education, n (%) | <0.001 | ||
| ≤High school | 98 (53.3) | 51 (26.6) | |
| >High school | 86 (46.7) | 141 (73.4) | |
| Clinical data | |||
| BMI ‡, median [IQR] kg/m2 | 26.7 [21.8 to 31.2] | 26.5 [22.2 to 30.5] | 0.83 |
| Age at menarche, median [IQR] years | 13 [12 to 14] | 13 [12 to 14] | 0.72 |
| Parity, median [IQR] | 2 [1 to 3] | 1 [0 to 2] | 0.007 |
| Hepatitis C virus infection, n (%) | <0.001 | ||
| Never | 96 (51.3) | 161 (84.3) | |
| Ever | 91 (48.7) | 30 (15.7) | |
| Tobacco smoking, n (%) | 0.004 | ||
| Never | 67 (35.6) | 89 (46.4) | |
| Past | 33 (17.6) | 45 (23.4) | |
| Current | 88 (46.8) | 58 (30.2) | |
| Substance use §, n (%) | 0.003 | ||
| Never | 101 (54.3) | 122 (63.9) | |
| Past | 41 (22.0) | 49 (25.7) | |
| Current | 44 (23.7) | 20 (10.5) | |
| HIV-related clinical data | |||
| Nadir CD4 count, n (%) | N/A ‖ | N/A | |
| <200 cells/mL | 50 (53.2) | ||
| 200–500 cells/mL | 40 (42.6) | ||
| >500 cells/mL | 4 (4.3) | ||
| Current CD4 count, n (%) | N/A | N/A | |
| <200 cells/mL | 22 (13.8) | ||
| 200–500 cells/mL | 42 (26.4) | ||
| >500 cells/mL | 95 (59.7) | ||
| Current HIV viral load, n (%) | N/A | N/A | |
| Undetectable (<40 copies/µL) | 155 (83.8) | ||
| Detectable (≥40 copies/µL) | 30 (16.2) | ||
| Highest ever HIV viral load, n (%) | N/A | N/A | |
| <100,000 copies/mL | 65 (46.4) | ||
| ≥100,000 copies/mL | 75 (53.6) | ||
| Years lived with HIV, median [IQR] | 19 [12 to 23] | N/A | N/A |
| Menopausal by Self-Report (n = 189) | Menopausal by Self-Report with Biochemical Confirmation (n = 175) | |||||
|---|---|---|---|---|---|---|
| Women Living with HIV (n = 91) | HIV-Negative Women (n = 98) | p-Value | Women Living with HIV (n = 83) | HIV-Negative Women (n = 92) | p-Value | |
| Socio-demographic characteristics | ||||||
| Age, median [IQR *] years | 55.9 [52.2 to 59.1] | 57.9 [54.0 to 62.9] | 0.03 | 56.8 [53.7 to 59.5] | 58.1 [53.9 to 62.9] | 0.13 |
| Ethnicity, n (%) | 0.26 | 0.19 | ||||
| White | 39 (42.9) | 50 (51.0) | 35 (42.2) | 49 (53.3) | ||
| Non-White | 52 (57.1) | 48 (49.0) | 48 (57.8) | 43 (46.7) | ||
| Income, n (%) | 0.001 | <0.001 | ||||
| <CAD 20,000 †/year | 51 (58.0) | 30 (32.6) | 46 (57.5) | 26 (29.5) | ||
| ≥CAD 20,000/year | 37 (42.0) | 62 (67.4) | 40 (49.4) | 68 (73.9) | ||
| Education, n (%) | 0.002 | 0.003 | ||||
| ≤High school | 46 (52.3) | 28 (28.6) | 41 (50.6) | 24 (26.1) | ||
| >High school | 42 (47.7) | 70 (71.4) | 40 (49.4) | 68 (73.9) | ||
| Clinical characteristics | ||||||
| BMI ‡, median [IQR] kg/m2 | 25.7 [20.8 to 31.2] | 26.0 [22.1 to 30.0] | 0.33 | 26.6 [20.9 to 31.2] | 26.4 [22.1 to 30.5] | 0.34 |
| Age at menarche, median [IQR] years | 13 [12 to 14] | 13 [12 to 14] | 0.21 | 13 [12 to 14] | 13 [12 to 14] | 0.13 |
| Age at menopause, median [IQR] years | 49.0 [45.3 to 53.0] | 50.0 [46.0 to 53.0] | 0.28 | 50.0 [46.0 to 53.0] | 51.0 [46.0 to 53.0] | 0.54 |
| Parity, median [IQR] | 2 [1 to 3] | 2 [0 to 3] | 0.08 | 2 [1 to 3] | 2 [0 to 2] | 0.15 |
| Hepatitis C virus infection, n (%) | <0.001 | <0.001 | ||||
| Never | 37 (40.7) | 82 (83.7) | 38 (45.8) | 79 (85.9) | ||
| Ever | 54 (59.3) | 16 (16.3) | 45 (54.2) | 13 (14.1) | ||
| Tobacco smoking, n (%) | 0.03 | 0.008 | ||||
| Never | 33 (36.3) | 46 (46.9) | 32 (38.6) | 46 (50.0) | ||
| Past | 16 (17.6) | 25 (25.5) | 15 (18.1) | 26 (28.3) | ||
| Current | 42 (46.2) | 27 (27.6) | 36 (43.4) | 20 (21.7) | ||
| Substance use §, n (%) | 0.03 | 0.008 | ||||
| Never | 53 (58.2) | 63 (64.3) | 51 (61.4) | 62 (67.4) | ||
| Past | 17 (18.7) | 26 (26.5) | 15 (18.1) | 25 (27.2) | ||
| Current | 21 (23.1) | 9 (9.2) | 17 (20.5) | 5 (5.4) | ||
| HIV-related variables | ||||||
| Nadir CD4 count, n (%) | N/A ‖ | N/A | N/A | N/A | ||
| <200 cells/mL | 27 (56.2) | 26 (60.5) | ||||
| 200–500 cells/mL | 20 (41.7) | 17 (39.5) | ||||
| >500 cells/mL | 1 (2.1) | 0 (0) | ||||
| Current CD4 count, n (%) | N/A | N/A | N/A | N/A | ||
| <200 cells/mL | 9 (11.2) | 8 (10.8) | ||||
| 200–500 cells/mL | 23 (28.7) | 21 (28.4) | ||||
| >500 cells/mL | 48 (60.0) | 45 (60.8) | ||||
| Current HIV viral load, n (%) | N/A | N/A | N/A | N/A | ||
| Undetectable (<40 copies/µL) | 78 (85.7) | 71 (85.5) | ||||
| Detectable (≥40 copies/µL) | 13 (14.3) | 12 (14.5) | ||||
| Highest HIV viral load, n (%) | N/A | N/A | N/A | N/A | ||
| <100,000 copies/µL | 31 (45.6) | 27 (45.0) | ||||
| ≥100,000 copies/µL | 37 (54.4) | 33 (55.0) | ||||
| Years lived with HIV, median [IQR] | 21 [15 to 25] | N/A | N/A | 21 [15 to 25] | N/A | N/A |
| Unadjusted β (95% CI) | p-Value | Adjusted β (95% CI) | p-Value | |
|---|---|---|---|---|
| HIV status (ref: HIV-negative) | −1.00 (−3.04 to 1.04) | 0.33 | 0.86 (−0.72 to 2.43) | 0.28 |
| Income (ref: ≥CAD 20,000/year) | −2.00 (−4.47 to 0.47) | 0.11 | 0.05 (−1.66 to 1.77) | 0.95 |
| Parity (per increase in one birth) | 0.00 (−0.71 to 0.71) | 1.00 | 0.00 (−0.54 to 0.54) | 0.99 |
| Body mass index (per one kg/m2 increase) | −0.00 (−0.10 to 0.10) | 1.00 | −0.04 (−0.14 to 0.06) | 0.41 |
| Hepatitis C virus infection (ref: never) | −2.00 (−4.45 to 0.45) | 0.11 | −1.00 (−2.94 to 0.94) | 0.31 |
| Tobacco smoking (ref: never) | ||||
| Past | 0.00 (−1.66 to 1.66) | 1.00 | −1.55 (−3.35 to 0.26) | 0.09 |
| Current | −3.00 (−4.95 to −1.05) | <0.001 | −2.62 (−5.48 to 0.24) | 0.07 |
| Substance use * (ref: never) | ||||
| Past | −1.00 (−2.72 to 0.72) | 0.25 | −0.31 (−2.31 to 1.68) | 0.76 |
| Current | −4.00 (−8.96 to 0.96) | 0.11 | −3.14 (−8.11 to 1.82) | 0.21 |
| Ethnicity (ref: White) | ||||
| Non-White | −1.00 (−2.88 to 0.88) | 0.29 | ||
| Age at menarche (per one-year increase) | −0.00 (−0.51 to 0.51) | 1.00 |
| Unadjusted β (95% CI) | p-Value | Adjusted β (95% CI) | p-Value | |
|---|---|---|---|---|
| Nadir CD4 count (ref: ≥200 cells/mL) | ||||
| <200 cells/mL | 0.00 (−7.76 to 7.76) | 1.00 | 0.00 (−5.33 to 5.33) | 1.00 |
| Current CD4 count (ref: ≥500 cells/mL) | ||||
| <500 cells/mL | −2.00 (−1.08 to 5.08) | 0.20 | 3.00 (−1.85 to 7.85) | 0.21 |
| Highest HIV viral load (ref: <100,000 copies/µL) | ||||
| ≥100,000 copies/mL | −1.00 (−4.39 to 2.39) | 0.56 | −2.00 (−9.33 to 5.33) | 0.58 |
| Current HIV viral load (ref: undetectable) | ||||
| Detectable | −2.50 (−5.99 to 0.99) | 0.16 | ||
| Years lived with HIV (per one-year increase) | −0.08 (−0.27 to 0.11) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swann, S.A.; King, E.M.; Tognazzini, S.; Campbell, A.R.; Levy, S.L.A.; Pick, N.; Prior, J.C.; Elwood, C.; Loutfy, M.; Nicholson, V.; et al. Age at Natural Menopause in Women Living with HIV: A Cross-Sectional Study Comparing Self-Reported and Biochemical Data. Viruses 2023, 15, 1058. https://doi.org/10.3390/v15051058
Swann SA, King EM, Tognazzini S, Campbell AR, Levy SLA, Pick N, Prior JC, Elwood C, Loutfy M, Nicholson V, et al. Age at Natural Menopause in Women Living with HIV: A Cross-Sectional Study Comparing Self-Reported and Biochemical Data. Viruses. 2023; 15(5):1058. https://doi.org/10.3390/v15051058
Chicago/Turabian StyleSwann, Shayda A., Elizabeth M. King, Shelly Tognazzini, Amber R. Campbell, Sofia L. A. Levy, Neora Pick, Jerilynn C. Prior, Chelsea Elwood, Mona Loutfy, Valerie Nicholson, and et al. 2023. "Age at Natural Menopause in Women Living with HIV: A Cross-Sectional Study Comparing Self-Reported and Biochemical Data" Viruses 15, no. 5: 1058. https://doi.org/10.3390/v15051058