
Efficacy and Safety of Upadacitinib for Management of Moderate-to-Severe Atopic Dermatitis: An Evidence-Based Review
 , ,
, ,
Abstract
:1. Introduction
2. Methods
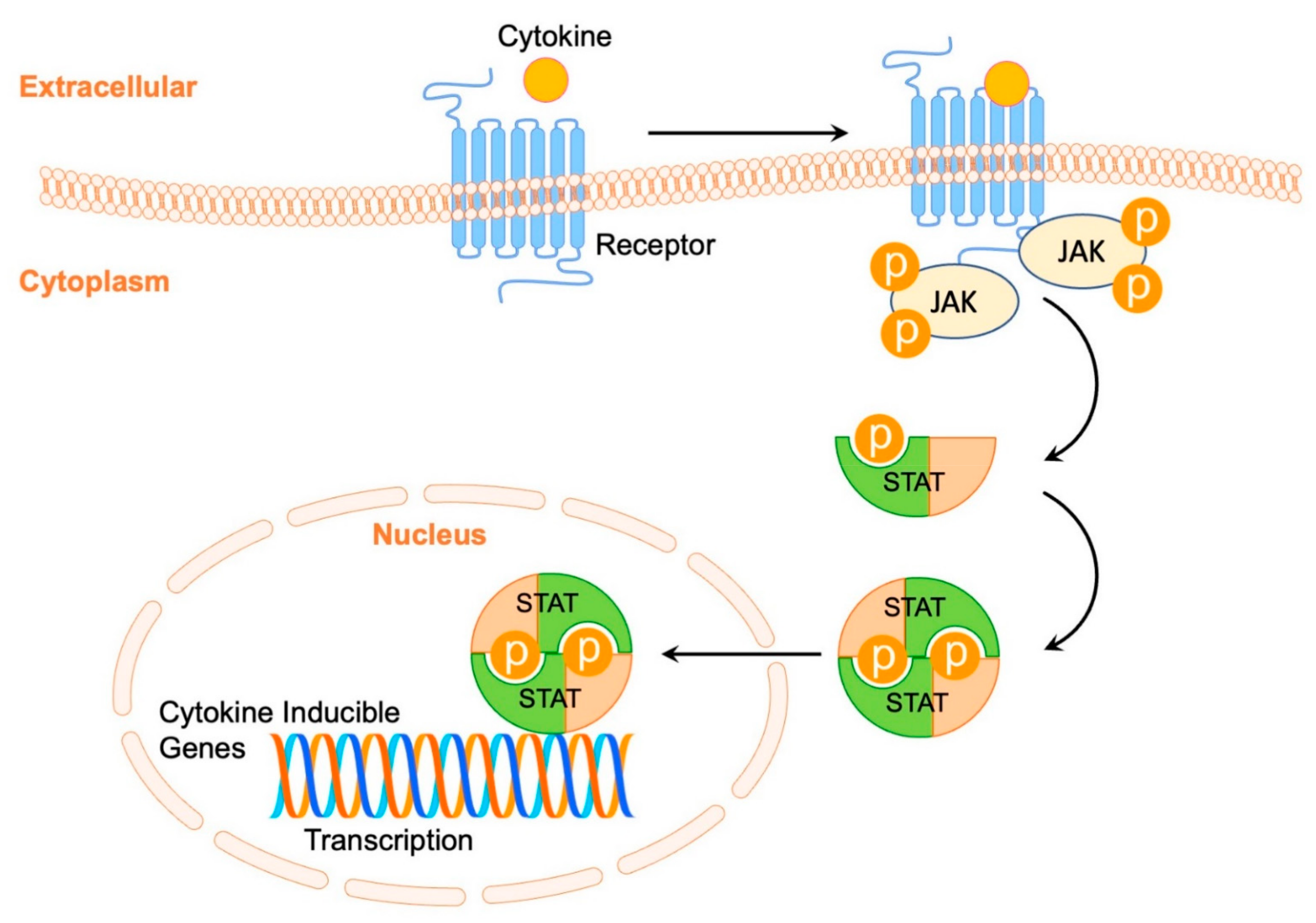
3. The Role of Janus Kinase-Signal Transducer in the Pathogenesis of Atopic Dermatitis
4. Upadacitinib in Atopic Dermatitis
5. Efficacy of Upadacitinib in Atopic Dermatitis Treatment
5.1. Phase II
5.2. Phase III
6. Safety of Upadacitinib in Atopic Dermatitis Treatment
7. Upadacitinib Compared to Available Treatment Options for Treatment of Atopic Dermatitis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deckers, I.A.; McLean, S.; Linssen, S.; Mommers, M.; van Schayck, C.P.; Sheikh, A. Investigigating international time trends in the incidence and prevalence of atopic eczema 1990–2010: A systematic review of epidemiological studies. PLoS ONE 2012, 7, e39803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, R.J.; Johns, N.E.; Williams, H.C.; Bolliger, I.W.; Dellavalle, R.P.; Margolis, D.J.; Marks, R.; Naldi, L.; Weinstock, M.A.; Wulf, S.K.; et al. The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions. J. Investig. Dermatol. 2014, 134, 1527–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bieber, T. Atopic dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Abuabara, K.; Henrickson, S.E.; Hoffstad, O.; Margolis, D.J. Increased Risk of Cutaneous and Systemic Infections in Atopic Dermatitis-A Cohort Study. J. Investig. Dermatol. 2017, 137, 1375–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollenberg, A.; Klein, E. Current aspects of innate and adaptive immunity in atopic dermatitis. Clin. Rev. Allergy Immunol. 2007, 33, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Rønnstad, A.T.M.; Halling-Overgaard, A.S.; Hamann, C.R.; Skov, L.; Egeberg, A.; Thyssen, J.P. Association of atopic dermatitis with depression, anxiety, and suicidal ideation in children and adults: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2018, 79, 448–456.e30. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, S.; Torres, T. Dupilumab for the Treatment of Atopic Dermatitis. Actas Dermo-Sifiliogr. 2018, 109, 230–240. [Google Scholar] [CrossRef]
- Lewis-Jones, S. Quality of life and childhood atopic dermatitis: The misery of living with childhood eczema. Int. J. Clin. Pract. 2006, 60, 984–992. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Thaçi, D.; Pangan, A.L.; Hong, H.C.; Papp, K.A.; Reich, K.; Beck, L.A.; Mohamed, M.F.; Othman, A.A.; Anderson, J.K.; et al. Upadacitinib in adults with moderate to severe atopic dermatitis: 16-week results from a randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2020, 145, 877–884. [Google Scholar] [CrossRef] [Green Version]
- Ring, J.; Alomar, A.; Bieber, T.; Deleuran, M.; Fink-Wagner, A.; Gelmetti, C.; Gieler, U.; Lipozencic, J.; Luger, T.; Oranje, A.P.; et al. Guidelines for treatment of atopic eczema (atopic dermatitis) part I. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1045–1060. [Google Scholar] [CrossRef]
- Roekevisch, E.; Spuls, P.I.; Kuester, D.; Limpens, J.; Schmitt, J. Efficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: A systematic review. J. Allergy Clin. Immunol. 2014, 133, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Baghoomian, W.; Na, C.; Simpson, E.L. New and Emerging Biologics for Atopic Dermatitis. Am. J. Clin. Dermatol. 2020, 21, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Hanifin, J.M. Adult eczema prevalence and associations with asthma and other health and demographic factors: A US population-based study. J. Allergy Clin. Immunol. 2013, 132, 1132–1138. [Google Scholar] [CrossRef]
- Simpson, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.P.; et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. N. Engl. J. Med. 2016, 375, 2335–2348. [Google Scholar] [CrossRef] [PubMed]
- Blauvelt, A.; de Bruin-Weller, M.; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.; Rubel, D.; et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): A 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 2017, 389, 2287–2303. [Google Scholar] [CrossRef]
- Thaçi, D.; Simpson, E.L.; Deleuran, M.; Kataoka, Y.; Chen, Z.; Gadkari, A.; Eckert, L.; Akinlade, B.; Graham, N.M.H.; Pirozzi, G.; et al. Efficacy and safety of dupilumab monotherapy in adults with moderate-to-severe atopic dermatitis: A pooled analysis of two phase 3 randomized trials (LIBERTY AD SOLO 1 and LIBERTY AD SOLO 2). J. Dermatol. Sci. 2019, 94, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef]
- Gittler, J.K.; Shemer, A.; Suárez-Fariñas, M.; Fuentes-Duculan, J.; Gulewicz, K.J.; Wang, C.Q.; Mitsui, H.; Cardinale, I.; de Guzman Strong, C.; Krueger, J.G.; et al. Progressive activation of T(H)2/T(H)22 cytokines and selective epidermal proteins characterizes acute and chronic atopic dermatitis. J. Allergy Clin. Immunol. 2012, 130, 1344–1354. [Google Scholar] [CrossRef] [Green Version]
- Kou, K.; Aihara, M.; Matsunaga, T.; Chen, H.; Taguri, M.; Morita, S.; Fujita, H.; Yamaguchi, Y.; Kambara, T.; Ikezawa, Z. Association of serum interleukin-18 and other biomarkers with disease severity in adults with atopic dermatitis. Arch. Dermatol. Res. 2012, 304, 305–312. [Google Scholar] [CrossRef]
- Kim, B.S.; Wang, K.; Siracusa, M.C.; Saenz, S.A.; Brestoff, J.R.; Monticelli, L.A.; Noti, M.; Tait Wojno, E.D.; Fung, T.C.; Kubo, M.; et al. Basophils promote innate lymphoid cell responses in inflamed skin. J. Immunol. 2014, 193, 3717–3725. [Google Scholar] [CrossRef]
- Seltmann, J.; Roesner, L.M.; von Hesler, F.W.; Wittmann, M.; Werfel, T. IL-33 impacts on the skin barrier by downregulating the expression of filaggrin. J. Allergy Clin. Immunol. 2015, 135, 1659–1661.e4. [Google Scholar] [CrossRef] [PubMed]
- Cole, C.; Kroboth, K.; Schurch, N.J.; Sandilands, A.; Sherstnev, A.; O’Regan, G.M.; Watson, R.M.; McLean, W.H.; Barton, G.J.; Irvine, A.D.; et al. Filaggrin-stratified transcriptomic analysis of pediatric skin identifies mechanistic pathways in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 82–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.Y.; Kim, C.R.; Huh, I.S.; Jung, M.Y.; Seo, E.Y.; Park, J.H.; Lee, D.Y.; Yang, J.M. Staphylococcus aureus Colonization in Acute and Chronic Skin Lesions of Patients with Atopic Dermatitis. Ann. Dermatol. 2013, 25, 410–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malajian, D.; Guttman-Yassky, E. New pathogenic and therapeutic paradigms in atopic dermatitis. Cytokine 2015, 73, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Renert-Yuval, Y.; Guttman-Yassky, E. What’s New in Atopic Dermatitis. Dermatol. Clin. 2019, 37, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Thepen, T.; Langeveld-Wildschut, E.G.; Bihari, I.C.; van Wichen, D.F.; van Reijsen, F.C.; Mudde, G.C.; Bruijnzeel-Koomen, C.A. Biphasic response against aeroallergen in atopic dermatitis showing a switch from an initial TH2 response to a TH1 response in situ: An immunocytochemical study. J. Allergy Clin. Immunol. 1996, 97, 828–837. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Silverberg, J.I.; Nemoto, O.; Forman, S.B.; Wilke, A.; Prescilla, R.; de la Peña, A.; Nunes, F.P.; Janes, J.; Gamalo, M.; et al. Baricitinib in adult patients with moderate-to-severe atopic dermatitis: A phase 2 parallel, double-blinded, randomized placebo-controlled multiple-dose study. J. Am. Acad. Dermatol. 2019, 80, 913–921.e9. [Google Scholar] [CrossRef] [PubMed]
- Wolk, K.; Witte, E.; Witte, K.; Warszawska, K.; Sabat, R. Biology of interleukin-22. Semin. Immunopathol. 2010, 32, 17–31. [Google Scholar] [CrossRef]
- Boniface, K.; Bernard, F.X.; Garcia, M.; Gurney, A.L.; Lecron, J.C.; Morel, F. IL-22 inhibits epidermal differentiation and induces proinflammatory gene expression and migration of human keratinocytes. J. Immunol. 2005, 174, 3695–3702. [Google Scholar] [CrossRef] [Green Version]
- Czarnowicki, T.; Malajian, D.; Shemer, A.; Fuentes-Duculan, J.; Gonzalez, J.; Suárez-Fariñas, M.; Krueger, J.G.; Guttman-Yassky, E. Skin-homing and systemic T-cell subsets show higher activation in atopic dermatitis versus psoriasis. J. Allergy Clin. Immunol. 2015, 136, 208–211. [Google Scholar] [CrossRef]
- Suárez-Fariñas, M.; Dhingra, N.; Gittler, J.; Shemer, A.; Cardinale, I.; de Guzman Strong, C.; Krueger, J.G.; Guttman-Yassky, E. Intrinsic atopic dermatitis shows similar TH2 and higher TH17 immune activation compared with extrinsic atopic dermatitis. J. Allergy Clin. Immunol. 2013, 132, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Ghoreschi, K.; Gadina, M. Jakpot! New small molecules in autoimmune and inflammatory diseases. Exp. Dermatol. 2014, 23, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Villarino, A.V.; Kanno, Y.; O’Shea, J.J. Mechanisms and consequences of Jak-STAT signaling in the immune system. Nat. Immunol. 2017, 18, 374–384. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, J.J.; Schwartz, D.M.; Villarino, A.V.; Gadina, M.; McInnes, I.B.; Laurence, A. The JAK-STAT pathway: Impact on human disease and therapeutic intervention. Annu. Rev. Med. 2015, 66, 311–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, E.B.; Sivaprasad, U. Th2 Cytokines and Atopic Dermatitis. J. Clin. Cell Immunol. 2011, 2, 110. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, J.J.; Kontzias, A.; Yamaoka, K.; Tanaka, Y.; Laurence, A. Janus kinase inhibitors in autoimmune diseases. Ann. Rheum Dis 2013, 72 (Suppl. 2), ii111–ii115. [Google Scholar] [CrossRef] [PubMed]
- Furue, K.; Ito, T.; Tsuji, G.; Ulzii, D.; Vu, Y.H.; Kido-Nakahara, M.; Nakahara, T.; Furue, M. The IL-13-OVOL1-FLG axis in atopic dermatitis. Immunology 2019, 158, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Pesu, M.; Laurence, A.; Kishore, N.; Zwillich, S.H.; Chan, G.; O’Shea, J.J. Therapeutic targeting of Janus kinases. Immunol. Rev. 2008, 223, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Hirahara, K.; Schwartz, D.; Gadina, M.; Kanno, Y.; O’Shea, J.J. Targeting cytokine signaling in autoimmunity: Back to the future and beyond. Curr. Opin. Immunol. 2016, 43, 89–97. [Google Scholar] [CrossRef]
- Alves de Medeiros, A.K.; Speeckaert, R.; Desmet, E.; Van Gele, M.; De Schepper, S.; Lambert, J. JAK3 as an Emerging Target for Topical Treatment of Inflammatory Skin Diseases. PLoS ONE 2016, 11, e0164080. [Google Scholar] [CrossRef]
- Shreberk-Hassidim, R.; Ramot, Y.; Zlotogorski, A. Janus kinase inhibitors in dermatology: A systematic review. J. Am. Acad. Dermatol. 2017, 76, 745–753.e19. [Google Scholar] [CrossRef] [PubMed]
- Damsky, W.; King, B.A. JAK inhibitors in dermatology: The promise of a new drug class. J. Am. Acad. Dermatol. 2017, 76, 736–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hald, A.; Andrés, R.M.; Salskov-Iversen, M.L.; Kjellerup, R.B.; Iversen, L.; Johansen, C. STAT1 expression and activation is increased in lesional psoriatic skin. Br. J. Dermatol. 2013, 168, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Oetjen, L.K.; Mack, M.R.; Feng, J.; Whelan, T.M.; Niu, H.; Guo, C.J.; Chen, S.; Trier, A.M.; Xu, A.Z.; Tripathi, S.V.; et al. Sensory Neurons Co-opt Classical Immune Signaling Pathways to Mediate Chronic Itch. Cell 2017, 171, 217–228.e3. [Google Scholar] [CrossRef] [Green Version]
- Parmentier, J.M.; Voss, J.; Graff, C.; Schwartz, A.; Argiriadi, M.; Friedman, M.; Camp, H.S.; Padley, R.J.; George, J.S.; Hyland, D.; et al. In vitro and in vivo characterization of the JAK1 selectivity of upadacitinib (ABT-494). BMC Rheumatol. 2018, 2, 23. [Google Scholar] [CrossRef] [Green Version]
- Winthrop, K.L. The emerging safety profile of JAK inhibitors in rheumatic disease. Nat. Rev. Rheumatol. 2017, 13, 320. [Google Scholar] [CrossRef] [Green Version]
- Klünder, B.; Mittapalli, R.K.; Mohamed, M.F.; Friedel, A.; Noertersheuser, P.; Othman, A.A. Population Pharmacokinetics of Upadacitinib Using the Immediate-Release and Extended-Release Formulations in Healthy Subjects and Subjects with Rheumatoid Arthritis: Analyses of Phase I-III Clinical Trials. Clin. Pharmacokinet. 2019, 58, 1045–1058. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, M.F.; Camp, H.S.; Jiang, P.; Padley, R.J.; Asatryan, A.; Othman, A.A. Pharmacokinetics, Safety and Tolerability of ABT-494, a Novel Selective JAK 1 Inhibitor, in Healthy Volunteers and Subjects with Rheumatoid Arthritis. Clin. Pharmacokinet. 2016, 55, 1547–1558. [Google Scholar] [CrossRef]
- Klünder, B.; Mohamed, M.F.; Othman, A.A. Population Pharmacokinetics of Upadacitinib in Healthy Subjects and Subjects with Rheumatoid Arthritis: Analyses of Phase I and II Clinical Trials. Clin. Pharmacokinet. 2018, 57, 977–988. [Google Scholar] [CrossRef] [Green Version]
- Guttman-Yassky, E.; Teixeira, H.D.; Simpson, E.L.; Papp, K.A.; Pangan, A.L.; Blauvelt, A.; Thaçi, D.; Chu, C.Y.; Hong, H.C.; Katoh, N.; et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): Results from two replicate double-blind, randomised controlled phase 3 trials. Lancet 2021, 397, 2151–2168. [Google Scholar] [CrossRef]
- Silverberg, J.I.; de Bruin-Weller, M.; Bieber, T.; Soong, W.; Kabashima, K.; Costanzo, A.; Rosmarin, D.; Lynde, C.; Liu, J.; Gamelli, A.; et al. Upadacitinib plus topical corticosteroids in atopic dermatitis: Week 52 AD Up study results. J. Allergy Clin. Immunol. 2022, 149, 977–987.e14. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Teixeira, H.D.; de Bruin-Weller, M.; Bieber, T.; Soong, W.; Kabashima, K.; Werfel, T.; Zeng, J.; Huang, X.; Hu, X.; et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): Results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2021, 397, 2169–2181. [Google Scholar] [CrossRef]
- Blauvelt, A.; Teixeira, H.D.; Simpson, E.L.; Costanzo, A.; De Bruin-Weller, M.; Barbarot, S.; Prajapati, V.H.; Lio, P.; Hu, X.; Wu, T.; et al. Efficacy and Safety of Upadacitinib vs Dupilumab in Adults with Moderate-to-Severe Atopic Dermatitis: A Randomized Clinical Trial. JAMA Dermatol. 2021, 157, 1047–1055. [Google Scholar] [CrossRef]
- Papp, K.A.; Menter, M.A.; Raman, M.; Disch, D.; Schlichting, D.E.; Gaich, C.; Macias, W.; Zhang, X.; Janes, J.M. A randomized phase 2b trial of baricitinib, an oral Janus kinase (JAK) 1/JAK2 inhibitor, in patients with moderate-to-severe psoriasis. Br. J. Dermatol. 2016, 174, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Smolen, J.S.; Weinblatt, M.E.; Burmester, G.R.; Meerwein, S.; Camp, H.S.; Wang, L.; Othman, A.A.; Khan, N.; Pangan, A.L.; et al. Efficacy and Safety of ABT-494, a Selective JAK-1 Inhibitor, in a Phase IIb Study in Patients with Rheumatoid Arthritis and an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2016, 68, 2857–2866. [Google Scholar] [CrossRef] [Green Version]
- Schmieder, G.J.; Draelos, Z.D.; Pariser, D.M.; Banfield, C.; Cox, L.; Hodge, M.; Kieras, E.; Parsons-Rich, D.; Menon, S.; Salganik, M.; et al. Efficacy and safety of the Janus kinase 1 inhibitor PF-04965842 in patients with moderate-to-severe psoriasis: Phase II, randomized, double-blind, placebo-controlled study. Br. J. Dermatol. 2018, 179, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Van Vollenhoven, R.F.; Fleischmann, R.; Cohen, S.; Lee, E.B.; García Meijide, J.A.; Wagner, S.; Forejtova, S.; Zwillich, S.H.; Gruben, D.; Koncz, T.; et al. Tofacitinib or adalimumab versus placebo in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 508–519. [Google Scholar] [CrossRef] [Green Version]
- Sandborn, W.J.; Ghosh, S.; Panes, J.; Vranic, I.; Su, C.; Rousell, S.; Niezychowski, W. Tofacitinib, an oral Janus kinase inhibitor, in active ulcerative colitis. N. Engl. J. Med. 2012, 367, 616–624. [Google Scholar] [CrossRef] [Green Version]
- Verden, A.; Dimbil, M.; Kyle, R.; Overstreet, B.; Hoffman, K.B. Analysis of Spontaneous Postmarket Case Reports Submitted to the FDA Regarding Thromboembolic Adverse Events and JAK Inhibitors. Drug Saf. 2018, 41, 357–361. [Google Scholar] [CrossRef]
- Gooderham, M.J.; Hong, H.C.; Eshtiaghi, P.; Papp, K.A. Dupilumab: A review of its use in the treatment of atopic dermatitis. J. Am. Acad. Dermatol. 2018, 78, S28–S36. [Google Scholar] [CrossRef]
- Bao, L.; Zhang, H.; Chan, L.S. The involvement of the JAK-STAT signaling pathway in chronic inflammatory skin disease atopic dermatitis. Jakstat 2013, 2, e24137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, P.M.; Guttman-Yassky, E.; Leung, D.Y. The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies. J. Allergy Clin. Immunol. 2017, 139, S65–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, E.L.; Sinclair, R.; Forman, S.; Wollenberg, A.; Aschoff, R.; Cork, M.; Bieber, T.; Thyssen, J.P.; Yosipovitch, G.; Flohr, C.; et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): A multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet 2020, 396, 255–266. [Google Scholar] [CrossRef]


{kind=link}
| Outcome | Medication and Dose | Guttman-Yassky et al. [9] (n = 167) | Measure Up 1 [50] (n = 847) | Measure Up 2 [50] (n = 836) | AD UP * [51,52] (n = 901) | Heads Up (n = 348) [53] | |
|---|---|---|---|---|---|---|---|
| Duration of treatment | 16 weeks | 16 weeks | 16 weeks | 16 weeks | 52 weeks | 16 weeks | |
| % of patients achieving EASI75 | Upadacitinib 7.5 mg | 29% done have SE | N/A | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 52% | 70% | 60% | 65% | 51% | ||
| Upadacitinib 30 mg | 69% | 80% | 73% | 77% | 69% | 71% | |
| Placebo | 10% | 16% | 13% | 26% | N/A | N/A | |
| Dupilumab 300 mg every other week | N/A | N/A | N/A | N/A | N/A | 61% | |
| % of patients achieving EASI90 | Upadacitinib 7.5 mg | 14% | N/A | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 26% | 53% | 42% | 43% | 38% | ||
| Upadacitinib 30 mg | 50% | 65.8% | 59% | 63% | 55% | 61% | |
| Placebo | 2% | 8.1% | 5% | 13% | N/A | ||
| Dupilumab 300 mg every other week | N/A | N/A | N/A | N/A | N/A | 39% | |
| % of patients achieving EASI100 | Upadacitinib 7.5 mg | 2.4% | N/A | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 9.5% | 17% | 14% | 12% | 13% | ||
| Upadacitinib 30 mg | 24% | 27% | 19% | 23% | 24% | 28% | |
| Placebo | 0% | 2% | 0.7% | 1.3% | N/A | N/A | |
| Dupilumab 300 mg every other week | N/A | N/A | N/A | N/A | N/A | 8% | |
| % improvement EASI | Upadacitinib 7.5 mg | 39% | N/A | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 62% | 80% | 74% | 78% | 68% | N/A | |
| Upadacitinib 30 mg | 74% | 88% | 85% | 87% | 77% | N/A | |
| Placebo | 23% | 41% | 35% | 46% | N/A | N/A | |
| Dupilumab 300 mg every other week | N/A | N/A | N/A | N/A | N/A | N/A | |
| % of patients achieving IGA 0/1 | Upadacitinib 7.5 mg | 14% | N/A | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 31% | 48% | 39% | 40% | 34% | N/A | |
| Upadacitinib 30 mg | 50% | 62% | 52% | 59% | 45% | N/A | |
| Placebo | 3% | 8% | 5% | 11% | N/A | N/A | |
| Dupilumab 300 mg every other week | N/A | N/A | N/A | N/A | N/A | N/A | |
| % of patients who achieved worst pruritus NRS improvement ≥ 4 | Upadacitinib 7.5 mg | 24% | N/A | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 59% | 60% | 60% | 51% | 45% | ||
| Upadacitinib 30 mg | 53% | 52% | 42% | 64% | 58% | 55% | |
| Placebo | 6% | 12% | 9% | 15% | N/A | N/A | |
| Dupilumab 300 mg every other week | N/A | N/A | N/A | N/A | N/A | 36% | |
| Adverse Event | Medication and Dose | Guttman-Yassky et al. [9] (n = 167) 16 Weeks | Measure Up 1 [50] (n = 847) 16 Weeks | Measure Up 2 [50] (n = 836) 16 Weeks | AD UP * [51,52] (n = 901) 16 Weeks | AD UP * [51,52] (n = 901) 52 Weeks |
|---|---|---|---|---|---|---|
| Any AE, n (%) | Upadacitinib 7.5 mg | 31(74) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 32 (76) | 176 (63) | 166 (60) | 200 (67) | 1730 (338) | |
| Upadacitinib 30 mg | 33 (79) | 209 (73) | 173 (61) | 215 (72) | 1848 (347) | |
| Placebo | 25 (63) | 166 (59) | 146 (53) | 190 (63) | N/A | |
| Serious AE, n (%) | Upadacitinib 7.5 mg | 2 (4.8) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 1 (2.4) | 6 (2) | 5 (2) | 7 (2) | 41 (8) | |
| Upadacitinib 30 mg | 0 (0) | 8 (3) | 7 (3) | 4 (1) | 43 (8) | |
| Placebo | 1 (2.5) | 8 (3) | 8 (3) | 9 (3) | N/A | |
| AE leading to drug discontinuation, n (%) | Upadacitinib 7.5 mg | 4 (9.5) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 2 (4.8) | 4 (1) | 11 (4) | 4 (1) | 20 (3.9) | |
| Upadacitinib 30 mg | 4 (9.5) | 11 (4) | 7 (3) | 4 (1) | 20 (3.8) | |
| Placebo | 3 (7.5) | 12 (4) | 12 (4) | 7 (2) | N/A | |
| Infection, n (%) | Upadacitinib 7.5 mg | 22 (52) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 18 (43) | 5 (2) | 9 (3) | 6 (2) | 28 (5.5) | |
| Upadacitinib 30 mg | 17 (41) | 9 (3) | 0 (0) | 9 (3) | 51 (9.6) | |
| Placebo | 8 (20) | 4 (1) | 0 (0) | 3 (1) | N/A | |
| Serious Infection, n (%) | Upadacitinib 7.5 mg | 2 (4.8) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 1 (2.4) | 2 (1) | 1 ( < 1) | 3 (1) | 14 (2.7) | |
| Upadacitinib 30 mg | 0 (0) | 2 (1) | 2 (1) | 0 (0) | 12 (2.3) | |
| Placebo | 0 (0) | 0 (0) | 2 (1) | 3 (1) | N/A | |
| Hepatic Disorder, n (%) | Upadacitinib 7.5 mg | 0 (0) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 2 (4.8) | 5 (2) | 2 (1) | 6 (2) | 41 (8) | |
| Upadacitinib 30 mg | 0 (0) | 8 (3) | 4 (1) | 3 (1) | 26 (5) | |
| Placebo | 1 (2.5) | 2 (1) | 4 (1) | 5 (2) | N/A | |
| Anemia, n (%) | Upadacitinib 7.5 mg | 0 (0) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 0 (0) | 1 ( < 1) | 2 (1) | 0 (0) | 7 (1.4) | |
| Upadacitinib 30 mg | 1 (2.4) | 8 (3) | 4 (1) | 3 (1) | 13 (2.4) | |
| Placebo | 0 (0) | 2 (1) | 4 (1) | 1 (0.3) | N/A | |
| Neutropenia, n (%) | Upadacitinib 7.5 mg | 1 (2.4) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 2 (4.8) | 4 (1) | 2 (1) | 2 (1) | 10 (2) | |
| Upadacitinib 30 mg | 2 (4.8) | 8 (3) | 4 (1) | 3 (1) | 15 (2.8) | |
| Placebo | 0 (0) | 2 (1) | 4 (1) | 0 (0) | N/A | |
| Lymphopenia, n (%) | Upadacitinib 7.5 mg | 0 (0) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 1 (2.4) | 1 ( < 1) | 0 (0) | 0 (0) | 2 (0.4) | |
| Upadacitinib 30 mg | 0 (0) | 2 (1) | 1 ( < 1) | 0 (0) | 1 (0.2) | |
| Placebo | 0 (0) | 2 (1) | 0 (0) | 1 (0.3) | N/A | |
| AE in ≥5% of patients in any group | N/A | N/A | N/A | N/A | N/A | |
| URTI, n (%) | Upadacitinib 7.5 mg | 7 (17) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 5 (12) | 25 (9) | 19 (7) | 21 (7) | 45 (10.2) | |
| Upadacitinib 30 mg | 5 (12) | 38 (13) | 17 (6) | 23 (8) | 45 (10.3) | |
| Placebo | 4 (10) | 20 (7) | 12 (4) | 22 (7) | N/A | |
| AD worsening, n (%) | Upadacitinib 7.5 mg | 6 (14) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 2 (4.8) | 9 (3) | 8 (3) | 11 (4) | 47 (11) | |
| Upadacitinib 30 mg | 4 (9.5) | 4 (1) | 4 (1) | 2 (1) | 29 (7) | |
| Placebo | 2 (5.0) | 26 (9) | 26 (9) | 20 (7) | N/A | |
| Acne, n (%) | Upadacitinib 7.5 mg | 4 (9.5) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 2 (4.8) | 19 (7) | 35 (13) | 30 (10) | 62 (14) | |
| Upadacitinib 30 mg | 6 (14) | 49 (17) | 41 (15) | 41 (14) | 81 (19) | |
| Placebo | 1 (2.5) | 6 (2) | 6 (2) | 6 (2) | N/A | |
| Headache, n (%) | Upadacitinib 7.5 mg | 3 (7.1) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 3 (7.1) | 14 (5) | 18 (7) | 15 (5) | 29 (7) | |
| Upadacitinib 30 mg | 4 (9.5) | 19 (7) | 20 (7) | 14 (5) | 28 (6) | |
| Placebo | 1 (2.5) | 12 (4) | 11 (4) | 15 (5) | N/A | |
| Nasopharyngitis, n (%) | Upadacitinib 7.5 mg | 2 (4.8) | N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 4 (9.5) | 22 (8) | 16 (6) | 37 (12) | 76 (17) | |
| Upadacitinib 30 mg | 3 (7.1) | 33 (12) | 18 (6) | 40 (13) | 73 (17) | |
| Placebo | 1 (2.5) | 16 (6) | 13 (5) | 34 (11) | N/A | |
| Blood CPK increased, n (%) | Upadacitinib 7.5 mg | 0 (0) | N/A N/A | N/A | N/A | N/A |
| Upadacitinib 15 mg | 3 (7.1) | 16 (6) | 9 (3) | 13 (4) | 37 (8) | |
| Upadacitinib 30 mg | 4 (9.5) | 16 (6) | 12 (4) | 18 (6) | 49 (11) | |
| Placebo | 2 (5.0) | 7 (3) | 5 (2) | 7 (2) |
| ClinicalTrials.gov | Phase | Patient Population | Interventions (Duration) | Primary Outcome |
|---|---|---|---|---|
| NCT03646604 | I | Pediatric [articipants (6–12 years) with severe AD (n = 32) | Upadacitinib (one dose) | Cmax Tmax AUCtau Oral Clearance Number of participants with treatment emergent adverse events |
| NCT03661138 (Rising Up) | III | Adolescents and adults (12–75 years) with moderate to severe atopic dermatitis (n = 272) | Upadacitinib or Placebo in Combination With Topical Corticosteroids (141 weeks) | Number of participants experiencing adverse events |
| NCT04195698 | III | Adults (18–75 years) with moderate to severe AD, successfully completed treatment with either Dupilumab or Upadacitinib (n = 485) | Upadacitinib (52 weeks) | Number of participants with adverse events |
| NCT05507580 (Flex-Up) | IIIb/IV | Adults (18–64 years) with moderate to severe AD (n = 600) | Upadacitinib (12 weeks, 24 weeks) | Percentage of participants achieving EASI 75 Percentage of participants achieving EASI 90 Percentage of participants achieving EASI 90 and WP-NRS of 0 or 1 |
| NCT05394792 (CAN UpTIMISE) | Observational Prospective | Adults with moderate-to-severe AD, inadequate responce or discontinuation of dupilumab (n = 100) | Upadacitinib (up to 4 months) | Percentage of participants achieving validated investigator Global assessment for atopic dermatitis vlGA-AD of 0 or 1 |
| NCT05139836 (UP-TAINED) | Observational Prospective | Adults with AD (n = 772) | Upadacitinib (up to 24 months) | Percentage of participants achieving disease control Defined by ADCT total score <7 points Percentage of participants achieving disease control Defined by ADCT total score <7 points among participants Who achieved disease control at month 3 |
| NCT05081557 (AD-VISE) | Observational Prospective | Adults and adolescents (≥12 Years Old) with AD 9 n = 975) | Upadacitinib (up to 24 months) | Upadacitinib utilization patterns vIGA-AD 0/1 vIGA-AD 0/1 among participants who achieved vIGA-AD 0/1 at Month 4 |
| NCT05029895 | Observational Prospective | Adolescents (≥12–18 Years) with AD (n = 170) | Upadacitinib (2 years) | Percentage of participants with serious infection |
| NCT05451316 (ADMIRE) | Observational Prospective | Adolescents and adults (≥12) with moderate to severe prurigo-type AD (n = 200) | Upadacitinib (up to 12 weeks) | Percentage of participants achieving WP-NRS reduction ≥ 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lytvyn, Y.; Mufti, A.; Abduelmula, A.; Sachdeva, M.; Maliyar, K.; Georgakopoulos, J.R.; Yeung, J. Efficacy and Safety of Upadacitinib for Management of Moderate-to-Severe Atopic Dermatitis: An Evidence-Based Review. Pharmaceutics 2022, 14, 2452. https://doi.org/10.3390/pharmaceutics14112452
Lytvyn Y, Mufti A, Abduelmula A, Sachdeva M, Maliyar K, Georgakopoulos JR, Yeung J. Efficacy and Safety of Upadacitinib for Management of Moderate-to-Severe Atopic Dermatitis: An Evidence-Based Review. Pharmaceutics. 2022; 14(11):2452. https://doi.org/10.3390/pharmaceutics14112452
Chicago/Turabian StyleLytvyn, Yuliya, Asfandyar Mufti, Abrahim Abduelmula, Muskaan Sachdeva, Khalad Maliyar, Jorge R. Georgakopoulos, and Jensen Yeung. 2022. "Efficacy and Safety of Upadacitinib for Management of Moderate-to-Severe Atopic Dermatitis: An Evidence-Based Review" Pharmaceutics 14, no. 11: 2452. https://doi.org/10.3390/pharmaceutics14112452