
Factors Associated with the Breast Cancer Diagnostic Interval across Five Canadian Provinces: A CanIMPACT Retrospective Cohort Study
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Diagnostic Interval
2.3. Study Variables
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Relevant Healthcare Administrative Data Codes
- -
- Histologically confirmed invasive breast cancer (behaviour = 3, ICD-0; 174.0–174.9 ICD-9)
- -
- * For patients with more than one cancer diagnoses in the same breast on the same day, select based on the order of the below criteria:Pick case with the highest stage;Pick case with highest histology priority;Pick case with the first malignancy number.
- -
- Breast cancer: OHIP: 174, 175 CIHI**: C50^
- -
- Other related cancer: OHIP: 162, 170, 173 195, 196, 197, 198, 199, CIHI: C34.90 C44.5 C76.1 C76.4 C77.3 C78.0 C78.2 C78.7 C79.2 C79.3^ C79.5^ C79.8^ C79.9 C80^
- -
- Benign breast neoplasm/CIS: OHIP: 214, 217, 229, 232, 233, 234, 238, 239 CIHI: D17.1 D24^ D04.5 D05^ D48.6^
- -
- Infectious/inflammatory conditions of the breast: OHIP: 610, 611 CIHI:N61
- -
- Breast biopsy (with/without ultrasound guidance): OHIP: J149, R107, X121, Z141, Z143, E525, E542 CCI: 2YK71, 2YM71, 2MD71, 3YM12 3YM94
- -
- Cyst aspiration or drainage: OHIP: Z118, Z139, Z140
- -
- Mastectomy—any type: OHIP: R105, R108, R109, R111, R117 CCI: 1YK87 1YL87 1YL89 1YM87 1YM89 1YM90 1YM91
- -
- Surgical consult with no procedure: OHIP: A035, A935
- -
- Bilateral mammography: X185 CCI: 3YM10
- -
- Diagnostic mammography and related procedures: X184, J004, J037, X192, X194, X201 CCI: 3YL10
- -
- Opportunistic screening mammogram: OHIP: X172↑↑, X178↑↑
- -
- Breast ultrasound: OHIP: J127, J427 CCI: 3YM30
- -
- Breast MRI: OHIP: X446, X447 and for 2007: X441, X445 CCI: 3YM40
- -
- Other ultrasound: J182, J195, J202, J425, J482, J502, CCI: 3GY30
- -
- Other MRI: X421, X425, (Post 2007: X441, X445), X471, X475, X490, X492, X499 CCI: 3AN40
- -
- Nuclear medicine: J650, J666, J667, J850 CCI: 3YM70
- -
- Abnormal mammogram within breast screening program: Screened = 2 (mammogram only) or 3 (yes, both PE and mammogram) and Finalres = C (breast cancer)
- -
- How codes were used:
- -
- Collected all breast-related diagnostic encounters listed above in 6 months from the diagnosis date (including the date of diagnosis).
- (1)
- For screening tests: In 6 months before (and including) the date of diagnosis, identify the earliest screening mammogram, including:
- -
- Abnormal mammograms within the breast screening program; and
- -
- Opportunistic screening mammograms
- (2)
- For diagnostic tests: In 6 months before (and including) the date of diagnosis, use OHIP and CIHI-DAD data, identify the earliest date of the last visits to referring physician who ordered the first test of each procedure below:
- -
- Diagnostic mammograms
- -
- Non-specific mammograms
- -
- Breast ultrasound
- -
- Breast MRI
- -
- Breast biopsy
- -
- Breast surgeon consultation PLUS codes for breast cancer, benign neoplasms/CIS or infectious/inflammatory conditions
- (3)
- For breast-related ED visits:
- -
- Breast cancer
- -
- Benign neoplasms/CIS
- -
- Infectious/inflammatory conditions, breast
- -
- Most recent healthcare encounter with referring physician prior to the first diagnostic test
- -
- The earliest date of breast-related encounters in 6 months before (including) the date of diagnosis

{kind=link}
{kind=link}
{kind=link}
| OHIP Code | Disease Diagnosis | ICD 10 Equivalent Code * |
|---|---|---|
| 162 | Lung neoplasm | C34.90 |
| 170 | Bone neoplasm | N/A ** |
| 173 | Other skin malignancies | C44.5 |
| 174 | Female breast neoplasm | C50 ^ |
| 175 | Male breast neoplasm | C50 ^ |
| 195 | Malignant neoplasms—Other ill defined sites | C76.1 C76.4 |
| 196 | Secondary neoplasms of lymph nodes | C77.3 |
| 197 | Secondary neoplasm of respiratory and digestive | C78.0 C78.2 C78.7 |
| 198 | Malignant neoplasms—metastatic or secondary, carcinoma | C79.2 C79.3 ^ C79.5 ^ C79.8 ^ C79.9 |
| 199 | Other malignant neoplasms | C80 ^ |
| 214 | Malignant neoplasms—lipoma | D17.1 |
| 217 | Benign neoplasms—breast | D24 ^ |
| 228 | [Haemangioma] and lymphangioma | N/A |
| 229 | Other benign neoplasms | N/A |
| 232 | CIS—Skin | D04.5 |
| 233 | CIS—Breast and [genito-urinary system] | D05^ |
| 234 | CIS—Other | N/A |
| 238 | Neoplasms uncertain behavior—other & unspecified sites | D48.6 ^ |
| 239 | Unspecified neoplasms eg polycythemia vera | N/A |
| 457 | Lymphedema, lymphangitis | N/A |
| 610 | Cystic mastitis, fibroadenosis of breast | N/A |
| 611 | Breast abscess, gynecomastia, hypertrophy, other breast | N/A |
| 683 | Acute lymphadenitis | L04.2 |
| A035 | General surgery consultation | |
| A935 | General surgery special surgery consultation | |
| E525 | Breast excision: Tumour or tissue for diagnostic biopsy and/or treatment, e.g.,carcinoma, fibroadenoma or fibrocystic disease after mammographic localization, add $ to R107 | |
| E542 | Needle biopsy when performed outside hospital, add $ to Z141 | |
| J004 | Embolization of spinal arteriovenous malformation: intramammary needling for localization under mammographic control | |
| J037 | Lymphangiogram: mammary ductography | |
| J127 | Diag US: scan B-mode (per breast) | 3YM30 |
| J149 | Ultrasonic guidance of biopsy, aspiration, amniocentesis or drainage procedures (one physician only) | |
| J182 | Diag US Extremities: per limb (excluding vascular study) | |
| J195 | Diag US Vascular: peri-art anal freq anal + scan—per limb Not in April 2013 OHIP Schedule | |
| J202 | Diag US Vascular: duplex scan i.e., simultaneous real time, B-mode imaging and frequency/spectral analysis, unilateral | |
| J425 | Diag US Thorax etc: Chest masses, pleural effusion—A & B-mode | 3GY30 |
| J427 | Diag US: scan B-mode (per breast) | 3ym30 needs to be here and look for other synonyms for the other CIHI codes |
| J482 | Diag US Extremities: per limb (excluding vascular study) | |
| J502 | Diag US Vascular: duplex scan i.e., simultaneous real time, B-mode imaging and frequency/spectral analysis, unilateral | |
| J650 | Nuclear Muskuloskeletal: bone scintigraphy general survey | |
| J666 | Nuclear Tomography: maximum one per Nuclear Medicine examination | 3YM70 |
| J667 | Nuclear Cardiovascular: first transit with blood pool images | |
| J850 | Nuclear Muskuloskeletal: bone scintigraphy general survey | |
| R105 | Breast excision: partial mastectomy plus radical node dissection Not in April 2013 OHIP Schedule | |
| R107 | Breast excision: Tumour or tissue for diagnostic biopsy and/or treatment, e.g.,carcinoma, fibroadenoma or fibrocystic disease | |
| R108 | Breast mastectomy—female w/wo biopsy—simple | 1YM89 1YM90 |
| R109 | Breast mastectomy—female w/wo biopsy—radical or modified radical | 1YM91 |
| R111 | Breast excision: partial mastectomy or wedge resection for treatment of breast disease, with or without biopsy, e.g., carcinoma or extensive fibrocystic disease | 1YK87 1YL87 1YL89 1YM87 |
| R117 | Breast mastectomy—female w/wo biopsy—subcutaneous with nipple preservation | |
| X121 | Xray special examinations: bronchogram stereotactic core breast biopsy | 3YM12 3YM94 |
| X172 * | Mammogram—no signs or symptoms—dedicated equipment—unilateral | |
| X178 * | Mammogram—no signs or symptoms—dedicated equipment—bilateral | |
| X184 ** | Mammogram—signs or symptoms—unilateral | |
| X185 ** | Mammogram—signs or symptoms—bilateral | 3YM10 |
| X192 | Xray: Misc exams—mammary ductography | 3YL10 |
| X194 * | Mammogram—no signs or symptoms—additional cone view w/wo magnification (limit two per breast) | |
| X201 | Mammogram—no signs or symptoms—breast biopsy specimen X-ray | |
| X421 | MRI head multislice sequence | 3AN40 |
| X425 | MRI head repeat | |
| X441 | MRI thorax multislice sequence | |
| X445 | MRI thorax repeat | |
| X446 | MRI breast—unilateral or bilateral—multislice sequence | 3YM40 |
| X447 | MRI breast—repeat | |
| X471 | MRI extremity or joint—multislice sequence | |
| X475 | MRI extremity or joint—repeat | |
| X490 | MRI limited spine—multislice sequence | |
| X492 | MRI limited spine—repeat | |
| X499 | MRI complex spine—3D MRI acquisition sequence | |
| Z118 | Skin/subcutaneous operation: foreign body removal—aspiration of superficial lump for cytology | |
| Z139 | Operations of the breast: aspiration of cyst—one or more | |
| Z140 | Operations of the breast: drainage of intramammary abscess or haematoma—single or multilocated—local anaesthetic | |
| Z141 | Operations of the breast: needle biopsy—one or more | 2YK71 2YM71 2MD71 |
| Z143 | Operations of the breast: needle biopsy—large core biopsy |
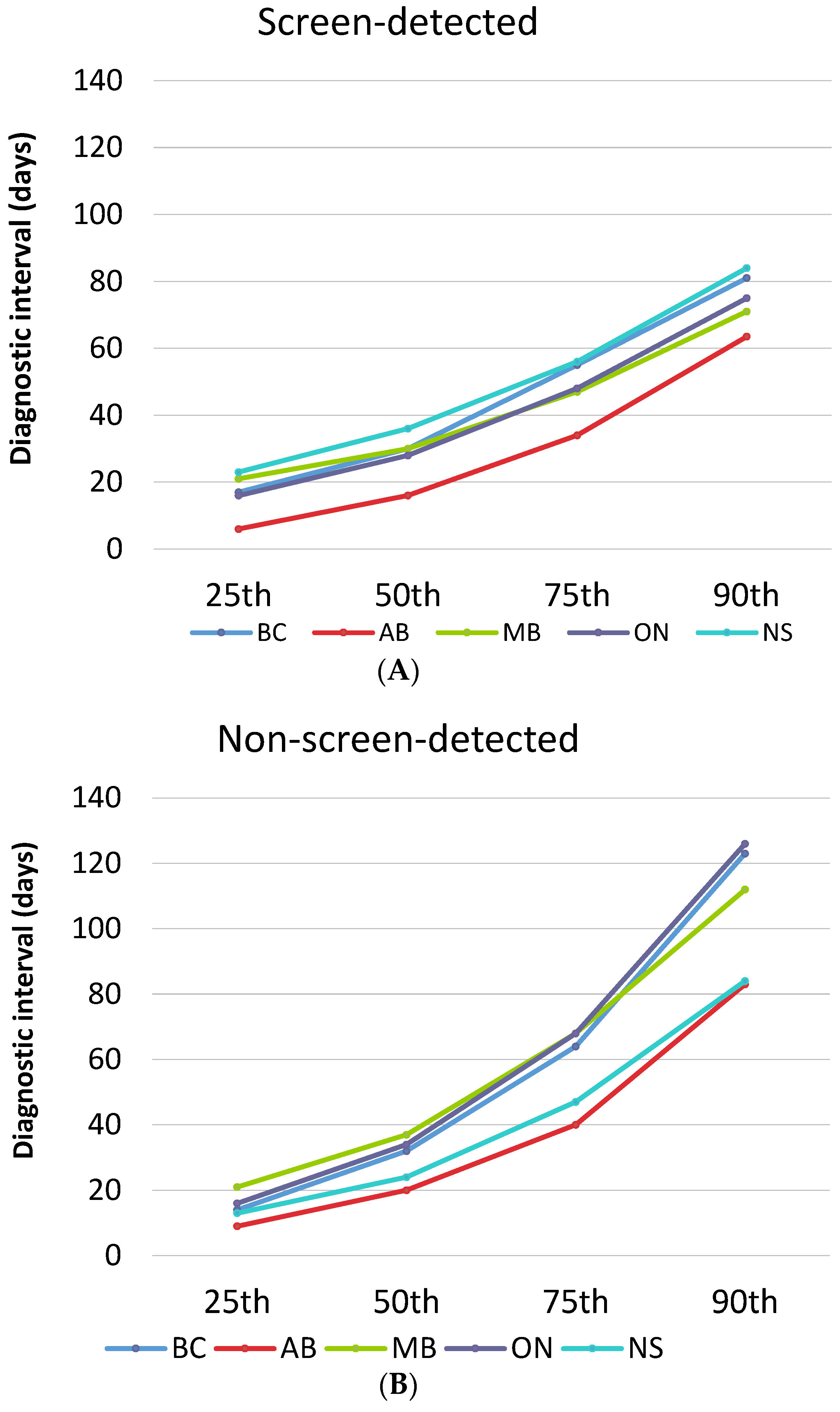
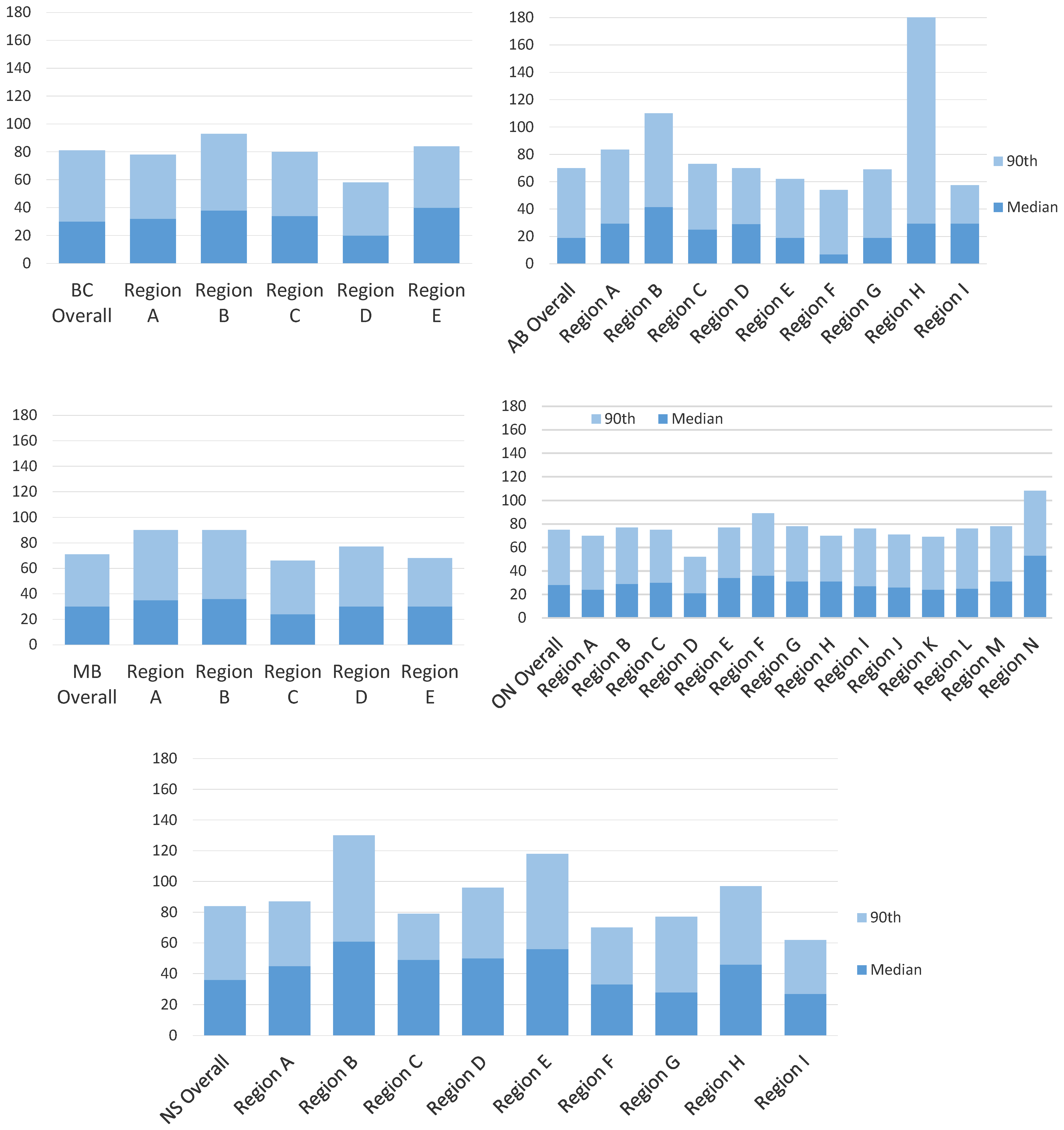
Appendix B. Intra-Provincial Variation for Screen-Detected Cancers

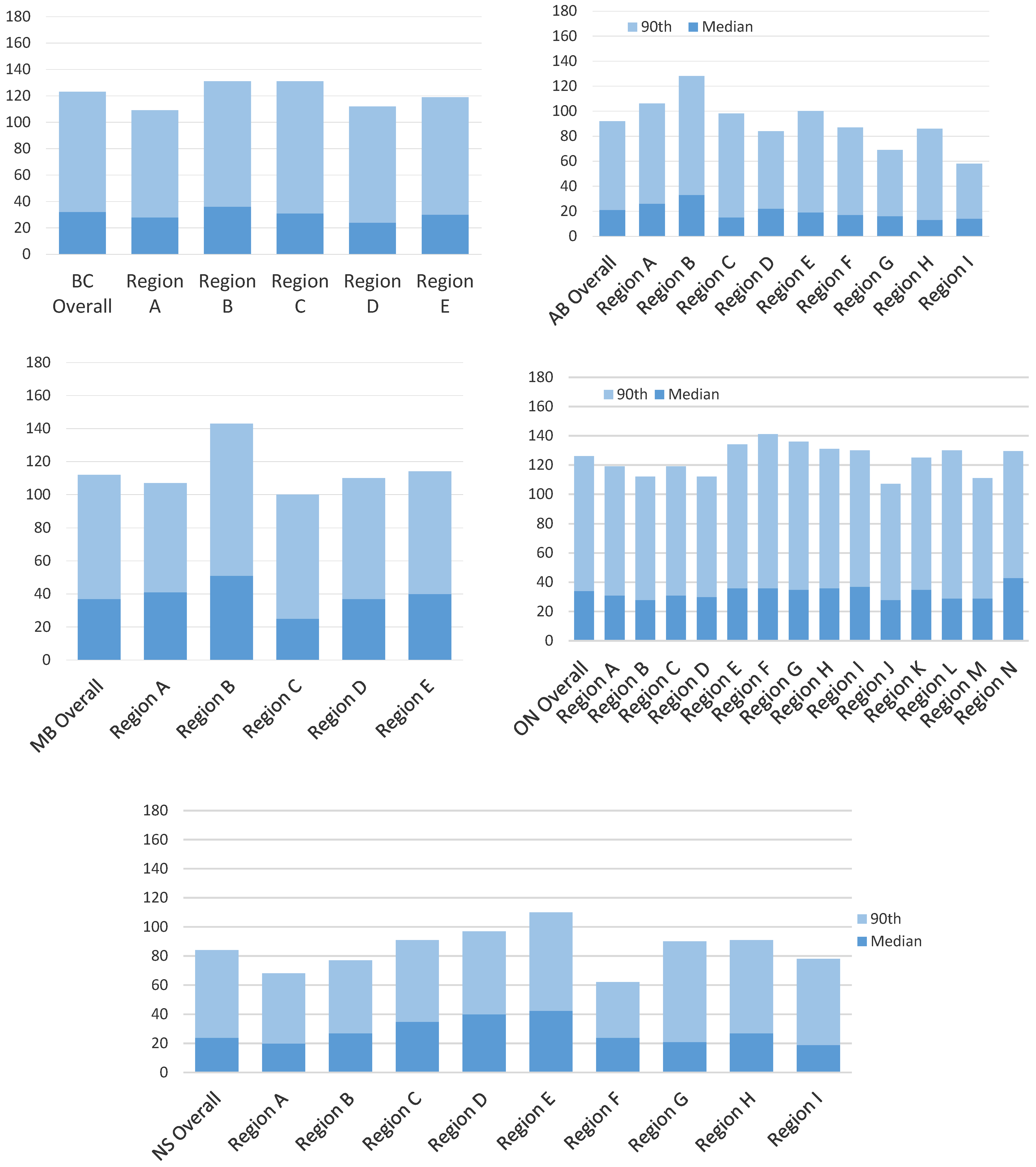
Appendix C. Intra-Provincial Variation for Non-Screened Cancers

Appendix D. Inter- and Intra-Provincial Variation in the Diagnostic Interval
| Screen-Detected Range (Days) | Non-Screen Detected Range (Days) | |||
|---|---|---|---|---|
| Median Range | 90th Range | Median Range | 90th Range | |
| Inter-provincial | 17 | 14 | 13 | 42 |
| British Columbia Intra-provincial | 20 | 35 | 22 | 22 |
| Alberta Intra-provincial | 34 | 127 | 20 | 30 |
| Manitoba Intra-provincial | 22 | 24 | 26 | 43 |
| Ontario Intra-provincial | 29 | 56 | 15 | 34 |
| Nova Scotia Intra-provincial | 29 | 56 | 24 | 48 |
References
- Bronner, M.B.; Nguyen, M.H.; Smets, E.M.A.; van de Ven, A.W.H.; van Weert, J.C.M. Anxiety during cancer diagnosis: Examining the influence of monitoring coping style and treatment plan. Psychooncology 2018, 27, 661–667. [Google Scholar] [CrossRef]
- Brocken, P.; Prins, J.B.; Dekhuijzen, P.N.R.; van der Heijden, H.F.M. The faster the better? A systematic review on distress in the diagnostic phase of suspected cancer, and the influence of rapid diagnostic pathways. Psychooncology 2012, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Neal, R.D.; Tharmanathan, P.; France, B.; Din, N.U.; Cotton, S.; Fallon-Ferguson, J.; Hamilton, W.; Hendry, A.; Hendry, M.; Lewis, R.; et al. Is increased time to diagnosis and treatment in symptomatic cancer associated with poorer outcomes? Systematic review. Br. J. Cancer 2015, 112 (Suppl. 1), S92–S107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caplan, L. Delay in Breast Cancer: Implications for Stage at Diagnosis and Survival. Front. Public Health 2014, 2, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Walker, M.J.; Meggetto, O.; Gao, J.; Espino-Hernández, G.; Jembere, N.; Bravo, C.A.; Rey, M.; Aslam, U.; Sheppard, A.J.; Lofters, A.K.; et al. Measuring the impact of the COVID-19 pandemic on organized cancer screening and diagnostic follow-up care in Ontario, Canada: A provincial, population-based study. Prev. Med. 2021, 151, 106586. [Google Scholar] [CrossRef] [PubMed]
- Canadian Partnership Against Cancer. Report from the Evaluation Indicators Working Group: Guidelines for Monitoring Breast Screening Program Performance; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2002. [Google Scholar]
- Marchildon, G.P.; Allin, S.; Merkur, S. Canada: Health System Review. Health Syst. Transit. 2020, 22, 1–194. [Google Scholar]
- Jiang, L.; Gilbert, J.; Langley, H.; Moineddin, R.; Groome, P.A. Effect of specialized diagnostic assessment units on the time to diagnosis in screen-detected breast cancer patients. Br. J. Cancer 2015, 112, 1744–1750. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Gilbert, J.; Langley, H.; Moineddin, R.; Groome, P.A. Is being diagnosed at a dedicated breast assessment unit associated with a reduction in the time to diagnosis for symptomatic breast cancer patients? Eur. J. Cancer Care 2018, 27, e12864. [Google Scholar] [CrossRef]
- Webber, C.; Jiang, L.; Grunfeld, E.; Groome, P.A. Identifying predictors of delayed diagnoses in symptomatic breast cancer: A scoping review. Eur. J. Cancer Care 2017, 26, e12483. [Google Scholar] [CrossRef] [PubMed]
- Groome, P.A.; McBride, M.L.; Jiang, L.; Kendell, C.; Decker, K.M.; Grunfeld, E.; Krzyzanowska, M.K.; Winget, M. Lessons Learned: It Takes a Village to Understand Inter-Sectoral Care Using Administrative Data across Jurisdictions. Int. J. Popul. Data Sci. 2018, 3, 440. [Google Scholar] [CrossRef] [PubMed]
- Grunfeld, E. It takes a team. Can. Fam. Physician 2016, 62, 781–782. [Google Scholar] [PubMed]
- Grunfeld, E. The two solitudes of primary care and cancer specialist care: Is there a bridge? Curr. Oncol. 2017, 24, 69–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winget, M.; Yuan, Y.; McBride, M.L.; Kendell, C.; Decker, K.M.; Grunfeld, E.; Groome, P.A. Inter- and intra-provincial variation in screen-detected breast cancer across five Canadian provinces: A CanIMPACT study. Can. J. Public Health 2020, 111, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Weller, D.; Vedsted, P.; Rubin, G.; Walter, F.M.; Emery, J.; Scott, S.; Campbell, C.; Andersen, R.S.; Hamilton, W.; Olesen, F.; et al. The Aarhus statement: Improving design and reporting of studies on early cancer diagnosis. Br. J. Cancer 2012, 106, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Li, M.; Yang, J.; Winget, M. Using administrative data to estimate time to breast cancer diagnosis and percent of screen-detected breast cancers—A validation study in Alberta, Canada. Eur. J. Cancer Care 2015, 24, 367–375. [Google Scholar] [CrossRef] [PubMed]
- The John Hopkins University. About the ACG System. Available online: https://www.hopkinsacg.org/about-the-acg-system/ (accessed on 2 January 2023).
- Austin, P.C.; van Walraven, C.; Wodchis, W.P.; Newman, A.; Anderson, G.M. Using the Johns Hopkins Aggregated Diagnosis Groups (ADGs) to predict mortality in a general adult population cohort in Ontario, Canada. Med. Care 2011, 49, 932–939. [Google Scholar] [CrossRef] [Green Version]
- Statistics Canada. Postal Code Conversion File (PCCF), Reference Guide; Statistics Canada: Ottawa, ON, Canada, 2017. [Google Scholar]
- Breslau, N.; Reeb, K.G. Continuity of care in a university-based practice. J. Med. Educ. 1975, 50, 965–969. [Google Scholar] [CrossRef]
- Crivellaro, P.; Tafur, M.; George, R.; Muradali, D. Diagnostic interval for non-screening patients undergoing mammography during the COVID-19 pandemic. Eur. Radiol. 2022, 32, 613–620. [Google Scholar] [CrossRef]
- Partridge, A.H.; Hughes, M.E.; Ottesen, R.A.; Wong, Y.-N.; Edge, S.B.; Theriault, R.L.; Blayney, D.W.; Niland, J.C.; Winer, E.P.; Weeks, J.C.; et al. The effect of age on delay in diagnosis and stage of breast cancer. Oncologist 2012, 17, 775–782. [Google Scholar] [CrossRef] [Green Version]
- Nnaji, C.A.; Ezenwankwo, E.F.; Kuodi, P.; Walter, F.M.; Moodley, J. Timeliness of diagnosis of breast and cervical cancers and associated factors in low-income and middle-income countries: A scoping review. BMJ Open 2022, 12, e057685. [Google Scholar] [CrossRef] [PubMed]
- Caplan, L.; May, D.; Richardson, L. Time to diagnosis and treatment of breast cancer: Results from the National Breast and Cervical Cancer Early Detection Program, 1991–1995. Am. J. Public Health 2000, 90, 130–134. [Google Scholar] [PubMed] [Green Version]
- Habbous, S.; Homenauth, E.; Barisic, A.; Kandasamy, S.; Majpruz, V.; Forster, K.; Yurcan, M.; Chiarelli, A.M.; Groome, P.; Holloway, C.M.B.; et al. Differences in breast cancer diagnosis by patient presentation in Ontario: A retrospective cohort study. C Open 2022, 10, E313–E330. [Google Scholar] [CrossRef] [PubMed]
- Chiarelli, A.M.; Muradali, D.; Blackmore, K.M.; Smith, C.R.; Mirea, L.; Majpruz, V.; O’Malley, F.P.; Quan, M.L.; Holloway, C.M.B. Evaluating wait times from screening to breast cancer diagnosis among women undergoing organised assessment vs. usual care. Br. J. Cancer 2017, 116, 1254–1263. [Google Scholar] [CrossRef] [Green Version]
- Plotogea, A.; Chiarelli, A.M.; Mirea, L.; Prummel, M.V.; Chong, N.; Shumak, R.S.; O’Malley, F.P.; Holloway, C.M.B.; Breast Screening Study Group. Clinical and prognostic factors associated with diagnostic wait times by breast cancer detection method. SpringerPlus 2014, 3, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivotto, I.A.; Gomi, A.; Bancej, C.; Brisson, J.; Tonita, J.; Kan, L.; Mah, Z.; Harrison, M.; Shumak, R. Influence of delay to diagnosis on prognostic indicators of screen-detected breast carcinoma. Cancer 2002, 94, 2143–2150. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.A.; Bancej, C.; Goel, V.; Snider, J.; McAuley, R.G.; Irvine, B.; Kan, L.; Mirsky, D.; Sabine, M.J.; McGilly, R.; et al. Waiting times from abnormal breast screen to diagnosis in 7 Canadian provinces. Can. Med. Assoc. J. 2001, 165, 277–283. [Google Scholar]
- Swanna, R.; McPhail, S.; Witt, J.; Shand, B.; Abel, G.A.; Hiom, S.; Rashbass, J.; Lyratzopoulos, G.; Rubin, G.; National Cancer Diagnosis Audit Steering Group. Diagnosing cancer in primary care: Results from the National Cancer Diagnosis Audit. Br. J. Gen. Pract. 2018, 68, e63–e72. [Google Scholar] [CrossRef]

| Variables | British Columbia | Alberta | Manitoba | Ontario | Nova Scotia |
|---|---|---|---|---|---|
| n = 4947 | n = 3780 | n = 1067 | n = 12,962 | n = 1525 | |
| Age | |||||
| <40 | 0 | 0 | 0 | 0.6 | 0 |
| 40–49 | 14 | 15.9 | 0.6 | 4 | 15.9 |
| 50–59 | 28.2 | 29.9 | 38.9 | 33.1 | 26.2 |
| 60–69 | 33.4 | 30.4 | 48.9 | 39.7 | 37.3 |
| 70–74 | 12.7 | 10.9 | 9.9 | 13.8 | 10.6 |
| 75+ | 11.7 | 12.9 | 1.7 | 8.8 | 10 |
| Co-morbidities | |||||
| 0–3 ADGs | 28.9 | - | 21 | 23.9 | 16.8 |
| 4–5 ADGs | 25.3 | 24.7 | 24.4 | 19.7 | |
| 6–7 ADGs | 22.1 | 21.7 | 22 | 22.9 | |
| 8–9 ADGs | 13.1 | 16.1 | 15.4 | 19.9 | |
| 10+ ADGs | 10.6 | 16.4 | 14.3 | 20.7 | |
| SES-Rurality | |||||
| High/Urban | 20.4 | 20.1 | 15.1 | 20.7 | 15.5 |
| Med/Urban | 53.5 | 48 | 43 | 52 | 40.1 |
| Low/Urban | 13.5 | 13 | 9.1 | 13.2 | 9.4 |
| High/Rural | 2.6 | 3.6 | 8 | 2.6 | 7.3 |
| Med/Rural | 7.3 | 11.2 | 20.7 | 8.3 | 21 |
| Low/Rural | 2.7 | 3.7 | 4.1 | 2.9 | 6.5 |
| Missing/Unknown | 0 | 0.3 | 0 | 0.3 | 0 |
| UPC index score | |||||
| 0 visits | 5.7 | 3.1 | 4.9 | 5.8 | 2.3 |
| 1–2 visits | 7.6 | 7.6 | 7.4 | 10.4 | 10.3 |
| UPC ≤ 0.75 (Low) | 40.2 | 44.9 | 36.5 | 25.1 | 25.1 |
| UPC > 0.75 (High) | 46.4 | 44.4 | 51.3 | 58.7 | 62.4 |
| Variables | British Columbia | Alberta | Manitoba | Ontario | Nova Scotia |
|---|---|---|---|---|---|
| n = 9251 | n = 7005 | n = 3017 | n = 31,475 | n = 2277 | |
| Age | |||||
| <40 | 6.2 | 8.5 | 6.2 | 6.7 | 6.3 |
| 40–49 | 18 | 23.8 | 20.5 | 22.9 | 16.6 |
| 50–59 | 21.7 | 24 | 19.2 | 22.2 | 19.5 |
| 60–69 | 21.5 | 17.6 | 17.7 | 19.5 | 20.1 |
| 70–74 | 8 | 7.3 | 9 | 7.6 | 9.6 |
| 75+ | 24.5 | 18.8 | 27.4 | 21.2 | 27.9 |
| Co-morbidities | |||||
| 0–3 ADGs | 33.8 | - | 24.6 | 26.3 | 25.3 |
| 4–5 ADGs | 23.7 | 21.8 | 22.5 | 21.7 | |
| 6–7 ADGs | 18.4 | 20.3 | 21.1 | 18.4 | |
| 8–9 ADGs | 12.8 | 16.2 | 15 | 14.6 | |
| 10+ ADGs | 11.3 | 17.1 | 15.1 | 19.9 | |
| SES-Rurality | |||||
| High/Urban | 17.6 | 16.4 | 14.8 | 19.6 | 11.9 |
| Med/Urban | 50.8 | 45.8 | 45 | 52.9 | 39.7 |
| Low/Urban | 18 | 14.3 | 12.9 | 15.6 | 12.2 |
| High/Rural | 2.7 | 4.1 | 5.5 | 2.2 | 5.8 |
| Med/Rural | 8.2 | 14.2 | 17.3 | 7.1 | 22.6 |
| Low/Rural | 2.6 | 4.6 | 4.3 | 2.2 | 7.6 |
| Missing/Unknown | 0 | 0.5 | 0 | 0.3 | 0 |
| UPC index score | |||||
| 0 visits | 7.4 | 6.5 | 6.6 | 7.2 | 7.2 |
| 1–2 visits | 8.3 | 8.4 | 9.2 | 10.8 | 13.7 |
| UPC ≤ 0.75 (Low) | 40 | 46.8 | 38.2 | 27.6 | 25.3 |
| UPC > 0.75 (High) | 44.4 | 38.4 | 45.9 | 54.4 | 53.8 |
| British Columbia | Alberta | Manitoba | Ontario | Nova Scotia | |
|---|---|---|---|---|---|
| n = 14,198 | n = 12,373 | n = 4216 | n = 44,437 | n = 3802 | |
| Screen-detected | |||||
| Median | 30 | 19 | 30 | 28 | 36 |
| IQR | 17–55 | NA | 21–47 | 16–48 | 23–56 |
| 90th % | 81 | 70 | 71 | 75 | 84 |
| Non-screen-detected | |||||
| Median | 32 | 21 | 37 | 34 | 24 |
| IQR | 14–64 | NA | 21–68 | 16–68 | 13–47 |
| 90th % | 123 | 92 | 112 | 126 | 85 |
| British Columbia | Alberta | Manitoba | Ontario | Nova Scotia | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Median | 90th | Median | 90th | Median | 90th | Median | 90th | Median | 90th |
| Intercept | 25 | 59 | 13 | 75 | 26.4 | 69 | 24 | 60 | NA | NA |
| Age | ||||||||||
| <40 | - | - | - | - | - | - | −11.3 | −18 | - | - |
| 40–49 | 3.0 | 7.2 | 2 | 22 | 8.8 | −1 | −5 | 28 | 0.1 | 15.8 |
| 50–59 | 1 | 0 | 1 | 1 | 2.8 | 2.5 | 0 | 3 | 0.7 | −1.9 |
| 60–69 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| 70–74 | 3 | −0.2 | 1 | 0.2 | −1.6 | −10 | 0.4 | 4 | −0.1 | −5.6 |
| 75+ | 0 | −4.2 | 1 | −3.3 | 4.5 | 13 | 0.6 | −2 | 3.3 | 0.8 |
| Co–morbidities | ||||||||||
| 0–3 ADGs | Ref | Ref | - ** | - ** | Ref | Ref | Ref | Ref | Ref | Ref |
| 4–5 ADGs | 1 | 1 | −1.2 | −15 | −1 | −3 | −1.1 | 5 | ||
| 6–7 ADGs | 0 | 3 | −0.8 | −11.5 | 0 | −3 | −2.4 | 7.4 | ||
| 8–9 ADGs | 2 | 7.6 | 1.8 | −5.5 | 1.4 | 1 | 0.4 | 14.6 | ||
| 10+ ADGs | 3 | 11.2 | −0.3 | −6 | 0 | 3 | 0.9 | 4.8 | ||
| SES–Rurality | ||||||||||
| High/Urban | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Med/Urban | −1 | 5.2 | 2 | −10.3 | 3.1 | 3 | 1.4 | 5 | −0.9 | −8.4 |
| Low/Urban | 1 | 16.6 | 2 | −12.3 | −0.5 | −4.5 | 1.4 | 3 | −5 | 13.4 |
| High/Rural | 0 | 12.4 | 8 | −10.3 | 1.6 | −2.5 | 3.3 | 15 | 10.4 | 0.3 |
| Med/Rural | 6 | 6.2 | 12 | −2.2 | 1.5 | 12.5 | 4 | 12 | 11.9 | 13.1 |
| Low/Rural | 10.2 | 0.8 | 11 | −8.7 | 5.3 | 14 | 5.4 | 17 | 19.3 | 26.6 |
| UPC index score | ||||||||||
| 0 visits | −5 | −6.2 | −3 | −1.8 | −3.5 | −4 | −1.4 | −2 | −8.6 | 8 |
| 1–2 visits | −1 | −1 | −1 | −3.8 | −2.5 | −5 | −2.6 | −8.6 | −3.3 | 1.1 |
| UPC < 0.75 | −1 | −0.4 | 0 | 5.2 | −1.5 | −3.5 | −1.4 | −1 | −1.3 | 15 |
| UPC > 0.75 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| British Columbia | Alberta | Manitoba | Ontario | Nova Scotia | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Median | 90th | Median | 90th | Median | 90th | Median | 90th | Median | 90th |
| Intercept | 25.6 | 98 | 19 | 72 | 35 | 102 | 28 | 104.7 | NA | NA |
| Age | ||||||||||
| <40 | 0 | −3 | 1 | −2.8 | −4 | −5 | 0.4 | −10.8 | ||
| 40–49 | 2.3 | 2 | −0.3 | 9 | 3.5 | 0.8 | 0 | 5 | 0.5 | 4 |
| 50–59 | 0.5 | 2.2 | 0.4 | 13 | 0.5 | −2.5 | 0 | 7.3 | −0.1 | −3 |
| 60–69 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| 70–74 | −1.3 | −6.6 | 1.7 | 13 | −1.5 | −20.8 | −1 | −12.7 | −2.2 | 6 |
| 75+ | −2 | −7.7 | −1 | −12 | −3.5 | −19 | −6 | −30 | −2.4 | −12.8 |
| Co–morbidities | ||||||||||
| 0–3 ADGs | Ref | Ref | - ** | - ** | Ref | Ref | Ref | Ref | Ref | Ref |
| 4–5 ADGs | 3.8 | 16.9 | 6.5 | 16.3 | 3 | 12 | −0.1 | 4.8 | ||
| 6–7 ADGs | 5.4 | 25.9 | 5.5 | 37.3 | 4 | 18 | 0.7 | 10.8 | ||
| 8–9 ADGs | 6.3 | 25.2 | 7.5 | 15.5 | 5 | 13.3 | 4.4 | 11.8 | ||
| 10+ ADGs | 7.9 | 36.7 | 8.5 | 15.5 | 7 | 23 | 4.5 | 24.8 | ||
| SES–Rurality | ||||||||||
| High/Urban | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Med/Urban | 1.2 | 3.8 | 0.2 | −5 | −1 | −9.8 | 2 | −3 | −2.2 | −8.3 |
| Low/Urban | 0.3 | −4.2 | −0.2 | −13 | 1 | −3.8 | 2 | −7.3 | −2.7 | −21 |
| High/Rural | −6.6 | 4.7 | −4.4 | −14 | −4.5 | −11.5 | 3 | 5 | 1.1 | −14 |
| Med/Rural | −2.8 | −2.2 | −0.1 | −11 | −5.5 | −6 | 0 | −3.3 | 3.3 | −13.8 |
| Low/Rural | −1.9 | −20.9 | −0.2 | −7 | −3 | 5.5 | −1 | −8 | 5.9 | 2 |
| UPC index score | ||||||||||
| 0 visits | −4.3 | −6.3 | −4.3 | −25 | −3.5 | −7.8 | −7 | −27.3 | −5.8 | 0.8 |
| 1–2 visits | −2.3 | −6.8 | −0.4 | −11 | 2.5 | 0 | −3 | −2 | −5 | 9.3 |
| UPC < 0.75 | −0.5 | 3.5 | 0.8 | 6 | −0.5 | 5 | 0 | 6.3 | 0.5 | 3.3 |
| UPC > 0.75 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruco, A.; Groome, P.A.; McBride, M.L.; Decker, K.M.; Grunfeld, E.; Jiang, L.; Kendell, C.; Lofters, A.; Urquhart, R.; Vu, K.; et al. Factors Associated with the Breast Cancer Diagnostic Interval across Five Canadian Provinces: A CanIMPACT Retrospective Cohort Study. Cancers 2023, 15, 404. https://doi.org/10.3390/cancers15020404
Ruco A, Groome PA, McBride ML, Decker KM, Grunfeld E, Jiang L, Kendell C, Lofters A, Urquhart R, Vu K, et al. Factors Associated with the Breast Cancer Diagnostic Interval across Five Canadian Provinces: A CanIMPACT Retrospective Cohort Study. Cancers. 2023; 15(2):404. https://doi.org/10.3390/cancers15020404
Chicago/Turabian StyleRuco, Arlinda, Patti A. Groome, Mary L. McBride, Kathleen M. Decker, Eva Grunfeld, Li Jiang, Cynthia Kendell, Aisha Lofters, Robin Urquhart, Khanh Vu, and et al. 2023. "Factors Associated with the Breast Cancer Diagnostic Interval across Five Canadian Provinces: A CanIMPACT Retrospective Cohort Study" Cancers 15, no. 2: 404. https://doi.org/10.3390/cancers15020404