 Alexander Moreno1,2,3*†
Alexander Moreno1,2,3*† Maria-Cristina Scola3,4†
Maria-Cristina Scola3,4† Hua Sun1,3
Hua Sun1,3 Henrick Durce1,3
Henrick Durce1,3 Célia Couve1,3
Célia Couve1,3 Kelly Acevedo1,3
Kelly Acevedo1,3 Gloria M. Gutman5
Gloria M. Gutman5- 1Department of Psychology, Université de Montréal, Montréal, QC, Canada
- 2Notre-Dame Hospital, Centre Intégré Universitaire de Santé et de Services Sociaux du Centre-Sud-de-l'Île-de-Montréal (CCSMTL), Montréal, QC, Canada
- 3Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, CIUSSS du Centre-Sud-de-l’Île-de-Montréal, Montréal, QC, Canada
- 4Department of Psychoeducation, Université de Montréal, Montréal, QC, Canada
- 5Gerontology Research Centre, Simon Fraser University, Vancouver, BC, Canada
Objective: Paucity of information concerning the efficacy of gerontechnologies to support aging in place among community-dwelling older adults prevents potential users, healthcare professionals, and policymakers from making informed decisions on their use. The goal of this study was to identify gerontechnologies tested for home support in dyads of community-dwelling older adults with unimpaired cognition and their family caregivers, including their benefits and challenges. We also provide the level of evidence of the studies and recommendations to address the specific challenges preventing their use, dissemination, and implementation.
Methods: We conducted a systematic review of the literature published between 2016 and 2021 on gerontechnologies tested for home support in dyads. Two independent reviewers screened the abstracts according to the inclusion/exclusion criteria. A third reviewer resolved eligibility discrepancies. Data extraction was conducted by two independent reviewers.
Results: Of 1,441 articles screened, only 13 studies met the inclusion criteria with studies of moderate quality. Mostly, these gerontechnologies were used to monitor the older adult or the environment, to increase communication with family caregivers, to assist in daily living activities, and to provide health information. Benefits included facilitating communication, increasing safety, and reducing stress. Common challenges included difficulties using the technologies, technical problems, privacy issues, increased stress and dissatisfaction, and a mismatch between values and needs.
Conclusion: Only a few gerontechnologies have proven efficacy in supporting community-dwelling older adults and their family caregivers. The inclusion of values and preferences, co-creation with end users, designing easy-to-use technologies, and assuring training are strongly recommended to increase acceptability and dissemination.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=310803, identifier CRD42022310803.
Introduction
In the past decades, the world population has shown a steady increase in the proportion of individuals aged 65 years and older. Approximately 10% of the world’s population is comprised of older adults (United Nations, 2021). This proportion is approximately double in Canada (18%) (StatCan, 2022) and other developed countries. This population trend poses worldwide challenges in the management of the health and well-being of older adults and their family caregivers.
Older adults prefer to live independently in their homes rather than in alternative living arrangements such as assisted living or long-term care (Kim, 2021). Independent living goes beyond a mere preference since it is linked to increased engagement with care service providers, self-determination, participation in problem-solving daily challenges, and improvement of mental health (Hurstfield et al., 2007). Considering these important benefits, governments around the world are shifting their policies to fund home and community-based services for older adults.
Older adults living with physical or cognitive difficulties may choose to move to a long-term care facility when they realize that there may be important risks for their health. Most older adults move to long-term care because they can no longer manage or be managed at home, and it is often someone else who makes the decision. The risk of social isolation, malnutrition, falls or other accidental injuries, as well as physical and cognitive deconditioning are important factors to consider (Moreland et al., 2012; Crichton et al., 2019; Fakoya et al., 2020; Di Lorito et al., 2021). For family caregivers, overload, burden, and compassion fatigue associated with high levels of chronic stress should be prevented or treated (Alves et al., 2019; Liao et al., 2022).
Different stakeholders including researchers, healthcare professionals, and the industry have been striving to develop technologies that can support older adults at home to promote their independence and autonomy. Gerontechnology is a transdisciplinary field using technologies (systems and equipment) to promote healthy aging and to solve problems related to chores, leisure, communication, and safety (Halicka, 2019). Gerontechnologies are used to prevent, delay, or compensate for physical, cognitive, and sensorial decline due to aging. For instance, gerontechnologies are used to optimize communication with family caregivers, monitor older adults and the environment to increase safety, and to assist in daily living activities (Colnar et al., 2020). At the same time, older adults can face barriers using technologies, particularly when they experience cognitive decline (Ikeda et al., 2021). For this reason, early intervention, familiarization, and progressive adaptation of these technologies can increase their impact. Family caregivers play an important role in the development, selection, and adoption of technologies to improve care in older adults (Leslie et al., 2021). A current paucity of information about the efficacy of these technologies prevents older adults, family caregivers, healthcare professionals, and policymakers from making informed decisions about their use.
Objective and research questions
The objective of this study was to evaluate and synthetize information via a systematic review of literature published between 2016 and 2021 concerning gerontechnologies used for home support among Community-Dwelling Older Adults (CDOA) without cognitive impairment and their Family Caregivers. The systematic review was designed to answer four main questions:
1. What gerontechnologies have been tested for home support by both CDOA and their family caregivers?
2. What are the benefits, challenges, and opportunities provided by these gerontechnologies for CDOA and their family caregivers?
3. What is the evidence level of the studies conducted with dyads comprised of CDOA and their family caregivers?
4. What recommendations, if any, address the specific challenges preventing the use and dissemination of these gerontechnologies?
Methods
Search strategy and information sources
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). A systematic review of literature published between 2016 and 2021 was conducted by the principal investigator (AM) in collaboration with two librarians with a background in Psychology and Geriatrics. The two librarians participated in different iterations and validations of the search strategy. Databases searched included: CINAHL, Medline, PsycINFO, Web of Science, and AgeLine. The search terms included « home support », « older adults », « family caregivers », and « technology ». Table 1 presents the search strategy, as well as truncation symbols (denoted by *) and Boolean operators (AND, OR). The systematic review was registered in PROSPERO (registration number: CRD42022310803).
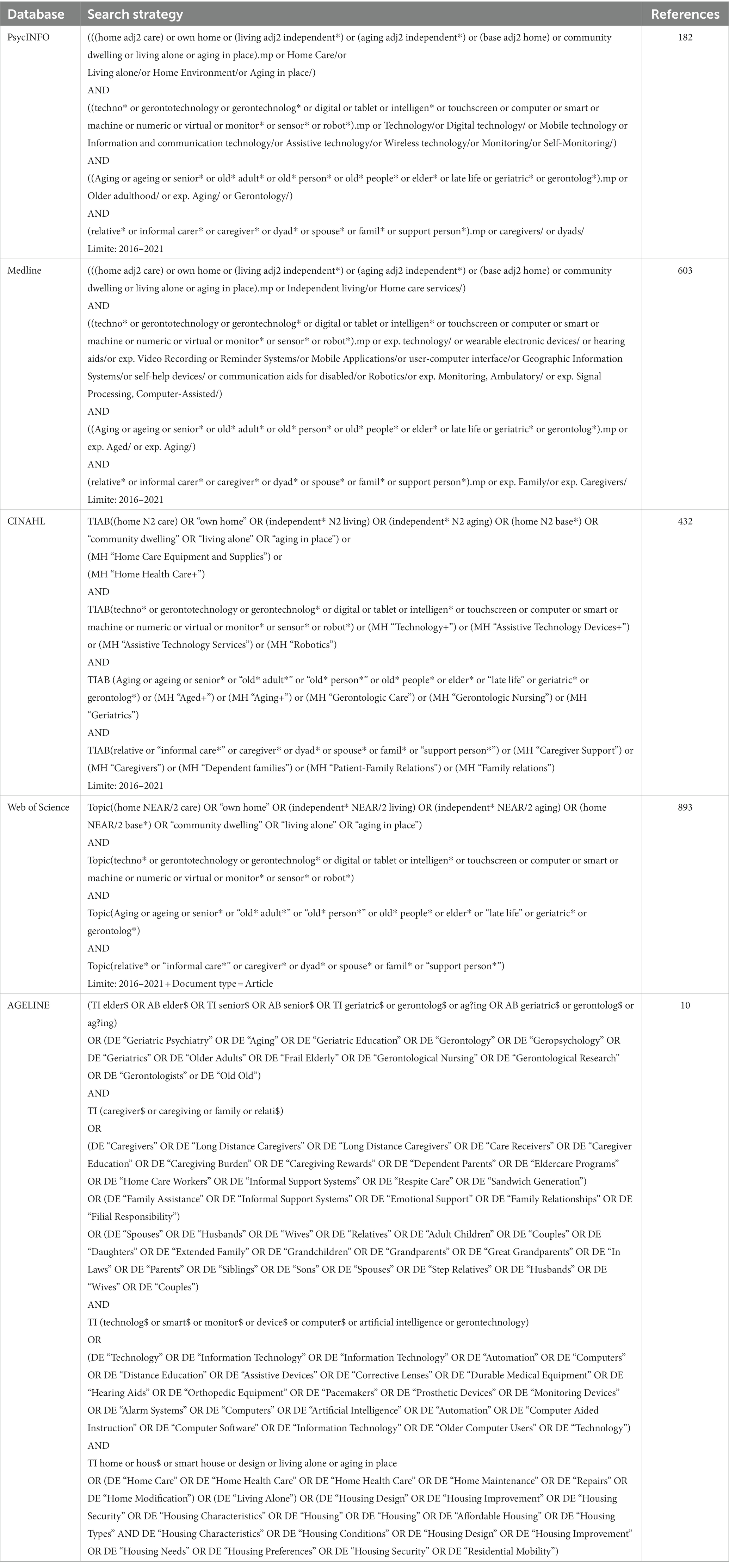
Table 1. Search terms and results from each database.
Study selection
Studies were included based on the following criteria: (a) studies reporting results on the efficacy or the feasibility of gerontechnologies tested at home; (b) gerontechnologies tested with dyads of CDOA and family caregivers; (c) tested with older adults without neurocognitive impairment; (d) studies using quantitative, qualitative or mixed data analysis methods; (e) studies available in Chinese, Spanish, French, or English. Studies were excluded if: (a) the sample included older adults with a diagnosis of cognitive impairment; (b) the gerontechnology was not tested with dyads of CDOA and family caregivers; (c) the gerontechnology did not provide in-home support; (d) the article was a research protocol; (e) the studies were available in languages other than Chinese, English, Spanish, or French. As shown in Figure 1, 2,120 references were identified. Two independent reviewers separately screened titles and abstracts based on inclusion/exclusion criteria (HS and KA) using COVIDENCE software (Veritas Health Innovation, 2014). Disagreements about inclusion were resolved by the supervisor (AM). A full-text review was then conducted for the remaining 109 references (HS and KA), with a total of 13 records compatible with the inclusion criteria.
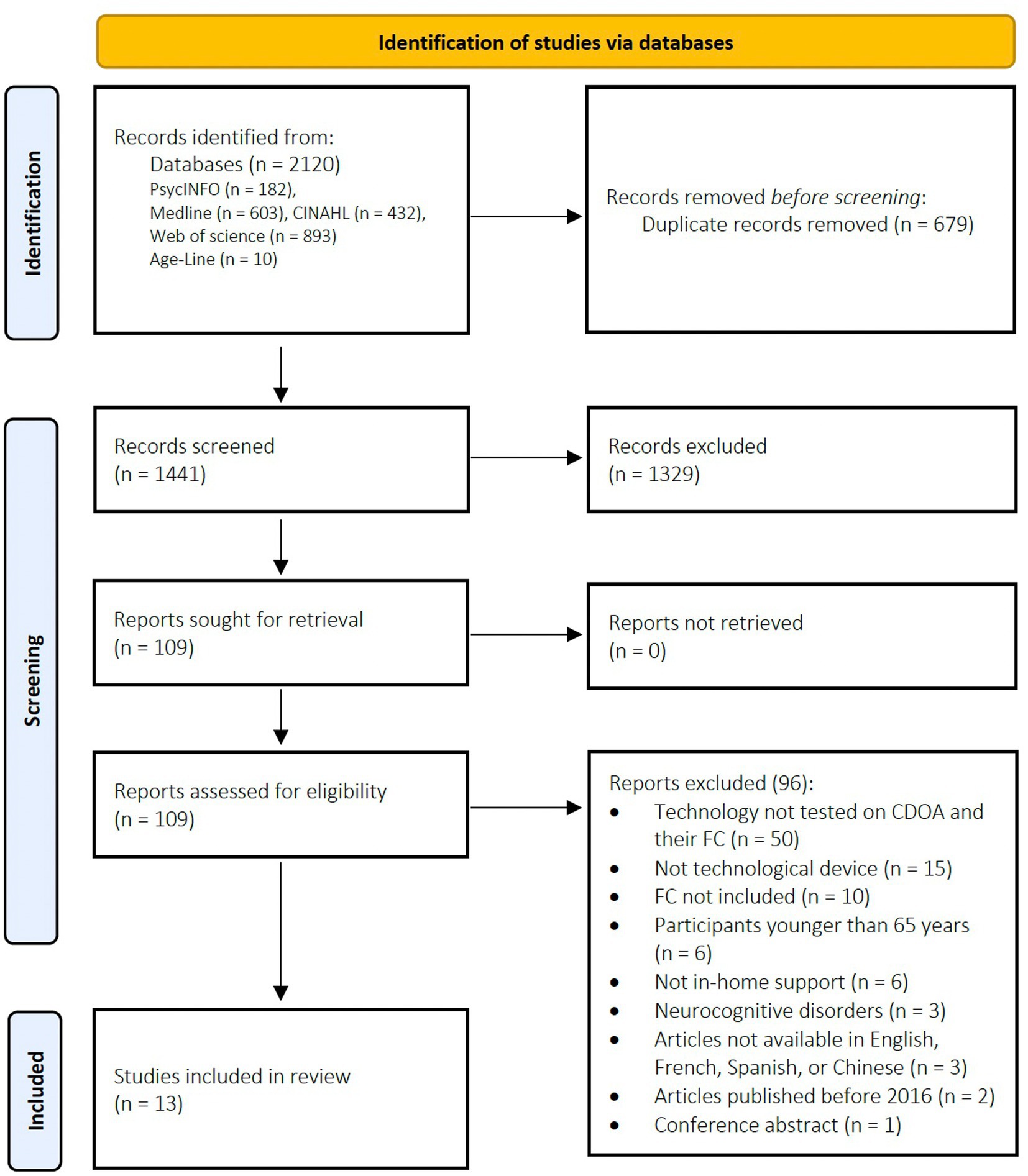
Figure 1. PRISMA flow diagram.
Data extraction and synthesis
Titles and abstracts were screened by two independent reviewers (students in psychology and a student with a background in engineering) according to the inclusion/exclusion criteria. Interrater reliability was assessed as moderate for the title and abstract screening (Cohen’s kappa coefficient of 0.48). Studies matching the inclusion criteria and those being unclear regarding their eligibility were retained for a full-text review. Interrater reliability was assessed as moderate for the full-text review (Cohen’s kappa coefficient of 0.51). A third reviewer (AM) resolved eligibility discrepancies where the first two reviewers did not reach a consensus. Data extraction was conducted by two independent reviewers, and included the sociodemographic characteristics of the participants, the characteristics of the gerontechnology tested at home, the duration of the intervention with the gerontechnology, the cost, and the benefits and challenges of using each specific gerontechnology.
Quality assessment
Three independent reviewers (HS, KA, M-CS) evaluated the quality of the empirical studies included in the present systematic review with the Mixed Methods Appraisal Tool (MMAT – Hong et al., 2018). This tool is designed for quality assessment of empirical studies included in systematic reviews. The scores range from 0 to 5, where scores near 5 indicate an excellent methodological quality. A mean score was calculated using the ratings of the three independent reviewers.
Results
A total of 13 studies met the study criteria and were included in this systematic review. Four studies used a qualitative method (Galambos et al., 2017; Åkerlind et al., 2018; Bradford et al., 2018; Berridge et al., 2019), six studies used a mixed-methods approach (Bock et al., 2016; Suzuki and Hasegawa, 2018; Grgurić et al., 2019; Gutierrez et al., 2019; Tseng and Hsu, 2019; Corbett et al., 2021), and three studies used quantitative methods (Cohen et al 2016; Quinn et al., 2019; Pais et al., 2020). Most studies were conducted in the United States (n = 5) (Bock et al., 2016; Galambos et al., 2017; Berridge et al., 2019; Quinn et al., 2019; Corbett et al., 2021). Other studies took place in Switzerland (n = 2) (Cohen et al., 2016; Pais et al., 2020), Sweden (n = 1) (Åkerlind et al., 2018), Australia (n = 1) (Bradford et al., 2018), Chile (n = 1) (Gutierrez et al., 2019), Croatia (n = 1) (Grgurić et al., 2019), Japan (n = 1) (Suzuki and Hasegawa, 2018), and Taiwan (n = 1) (Tseng and Hsu, 2019). The collective sample of these 13 studies included 172 older adults, with a mean age of 78.5 years (SD = 7.6), and 134 caregivers with a mean age of 51.7 (SD = 7). Gender, the relationship with the family caregiver, and the caregiving situation were not systematically reported in all of the studies. For the studies reporting them, the majority included mostly females in both the older adults and family caregivers’ groups. The family caregivers were mostly daughters. Only one study reported living arrangement, specifically, that 91.2% of the participants lived alone (Cohen et al., 2016). The technologies addressed different problems including the detection of medical emergencies (Åkerlind et al., 2018), falls (Galambos et al., 2017), or health issues (Cohen et al., 2016), the early detection of difficulties performing activities at home (Bradford et al., 2018), the lack of access to information or entertainment (Corbett et al., 2021), the need for rapid action when there are behavioral anomalies in older adults’ routines (Grgurić et al., 2019), social isolation (Gutierrez et al., 2019), medication compliance (Suzuki and Hasegawa, 2018), and lack of intergenerational connection between older adults and their adult children (Tseng and Hsu, 2019).
Level of evidence of the studies
The results of the Mixed Methods Appraisal Tool (MMAT) revealed that studies had on average a moderate quality of evidence (Table 2). The mean score obtained by the three independent reviewers was 3.7 (SD = 1). Common factors limiting the quality of the studies were linked to the sample sizes. Notably, all samples were small, a few had a high rate of attrition and a potential selection bias. For example, in Bradford et al. (2018), participants selected themselves (self-selection), thus it was mentioned that it is possible that they were already prone to positively appreciate the technology. In another study, most caregivers earned more than 100,000 US$ per year, which is considerably higher than the mean American salary (Quinn et al., 2019). Also, for the studies using a mixed methods design, divergences between qualitative and quantitative results were often not addressed (e.g., Grgurić et al., 2019).
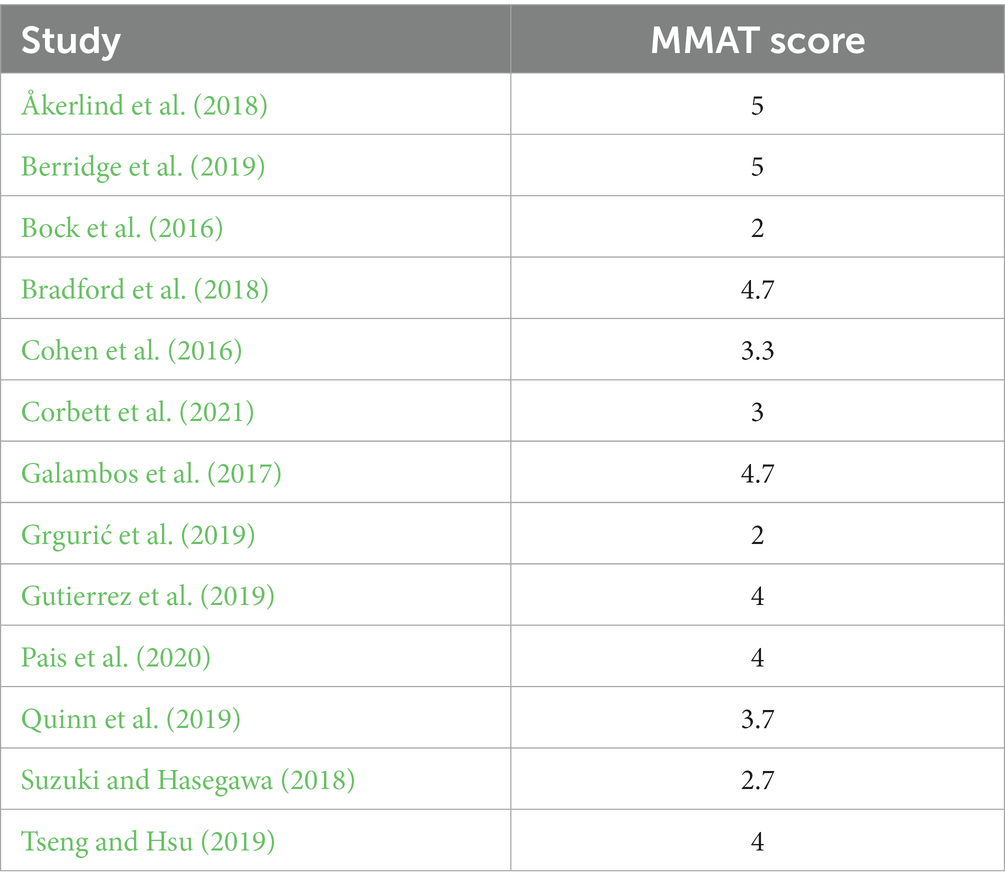
Table 2. Average scores of the Mixed Methods Appraisal Tool for the studies included in the systematic review.
Description of gerontechnologies for home-support tested simultaneously with community-dwelling older adults and their family caregivers
Each of the 13 studies evaluated a different technology. The mean duration of the intervention was 11.3 months (SD = 20.3) for a total of 135.5 months of intervention combining the 13 studies. Interventions varied in terms of their duration between 1 week and 6 years. A review of these technologies and their functionalities is presented in Tables 3 and 4.
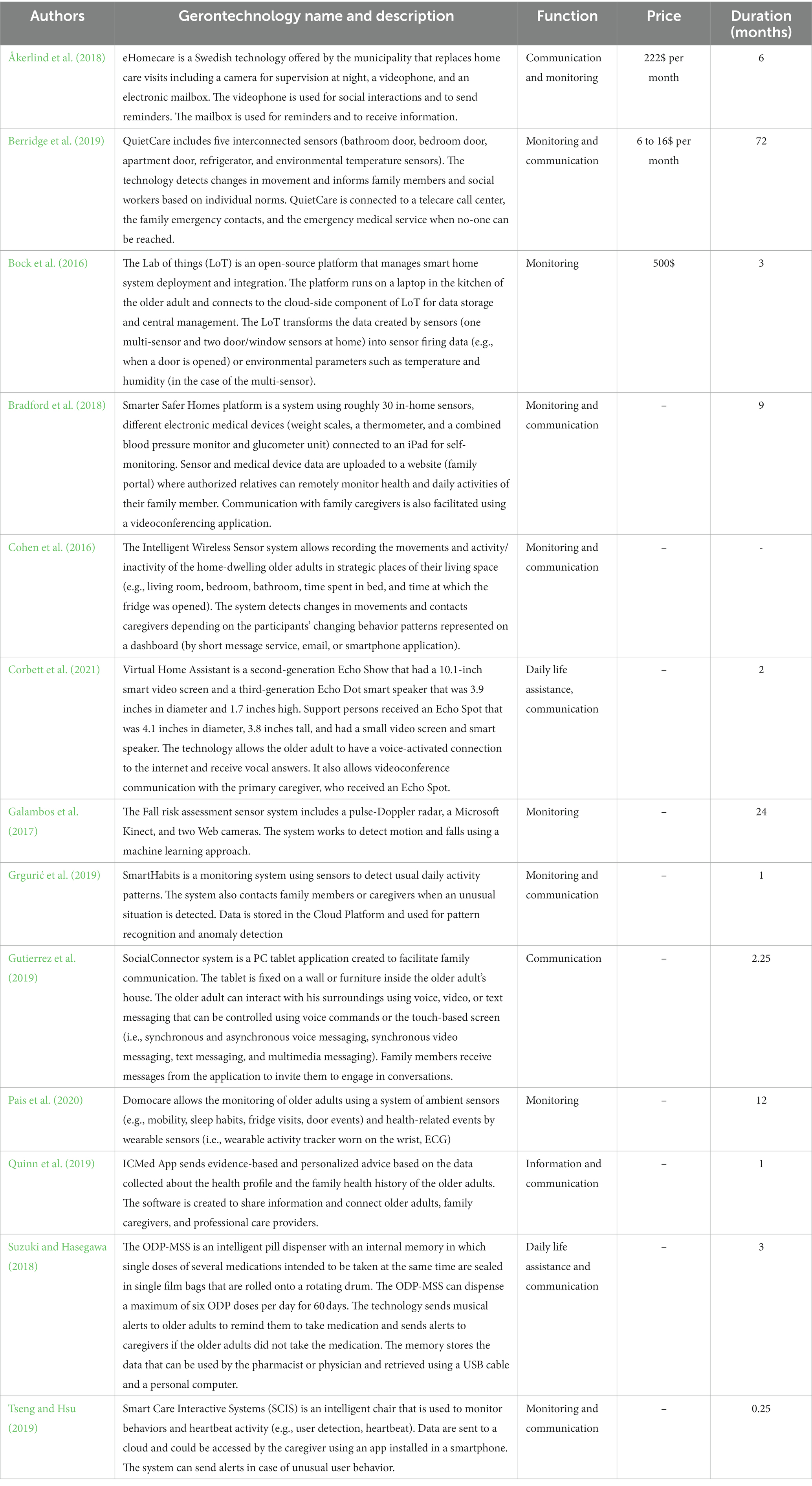
Table 3. Description of gerontechnologies for home-support tested simultaneously in community-dwelling older adults and their Family Caregivers.
In terms of functionalities, the technologies tested with CDOA and their family caregivers can be summarized as: (a) monitoring technologies, (b) communication technologies, (c) daily life assistance technologies, and (d) health information technologies.
Table 4. Characteristics and main findings of the studies included in the systematic review.
Monitoring technologies
Monitoring technologies are developed for supervision and to allow rapid detection of anomalies or dangers at home to ensure the safety of older adults. Most technologies (10/13) included a system to monitor individuals or the environment (Bock et al., 2016; Cohen et al., 2016; Galambos et al., 2017; Åkerlind et al., 2018; Bradford et al., 2018; Suzuki and Hasegawa, 2018; Berridge et al., 2019; Grgurić et al., 2019; Tseng and Hsu, 2019; Pais et al., 2020). Cameras and sensors were the most widely used monitoring technologies in these studies. Cameras were used to monitor older adults in bed during nighttime (Åkerlind et al., 2018) and to detect falls while older adults were walking in their homes (Galambos et al., 2017). Sensors were used to detect motion and record usual activity patterns (Bock et al., 2016; Cohen et al., 2016; Bradford et al., 2018; Berridge et al., 2019; Grgurić et al., 2019; Pais et al., 2020). For example, the Intelligent Wireless Sensor System (IWSS) consists of a set of sensors that record older adults’ movements in different rooms of their homes. Messages are sent to family caregivers when there is a behavioral pattern modification (Cohen et al., 2016). Four technologies used a system of alerts to signal anomalies (e.g., fall detection or change in walking pattern) (Galambos et al., 2017; Berridge et al., 2019; Grgurić et al., 2019; Tseng and Hsu, 2019) or to confirm that an activity has been performed by the older adult (e.g., self-administration of medication) (Suzuki and Hasegawa, 2018). Alerts were sent by the system and received by the family caregivers through text messaging and phone calls.
Communication technologies
A few technologies are designed to enhance the communication between the older adult living at home and their family caregivers. Five studies presented technologies serving this goal (Åkerlind et al., 2018; Bradford et al., 2018; Gutierrez et al., 2019; Quinn et al., 2019; Corbett et al., 2021). Smarter Safer Homes (Bradford et al., 2018) and the ICMed technology (Quinn et al., 2019) allowed the sharing of information about the health and daily activities between the older adult and the family caregiver via a platform. Finally, four technologies included a system of communication via phone calls, videoconferencing and/or text messages to connect older adults with their social circle (Åkerlind et al., 2018; Bradford et al., 2018; Gutierrez et al., 2019; Corbett et al., 2021). This allowed family caregivers to communicate in real time, do check-ups, and provide reminders when needed.
Daily life assistive technologies
A few technologies are designed to assist older adults in their daily life. These technologies include any electronic tool or equipment designed to help a person perform their regular daily activities, such as cooking, cleaning, entertaining, or planning. Two technologies served this purpose, namely the Virtual Home Assistant and the One-dose package medication support system. The Virtual Home Assistant is an electronic tablet used for entertainment, information search, planning (e.g., access to the calendar), and communication (Corbett et al., 2021). The One-dose package medication support system was used to help with medication compliance (Suzuki and Hasegawa, 2018).
Health information
Some technologies or applications are developed to increase access to evidence-based information that can help both older adults and their family caregivers manage their health and well-being. ICMed is a mobile application serving this goal. It uses the information collected on the older adult and their families to generate personal health advice (Quinn et al., 2019).
Benefits using gerontechnologies
Gerontechnologies have the potential to help CDOA maintain their autonomy and age in place when they are developed to respond to the specific needs of dyads. A review of the benefits found in the studies included: (a) increased communication and family participation, (b) increased sense of safety, (c) reduced stress of family members and CDOA, and (d) other perceived benefits.
Increased communication and family participation
Several studies revealed that the use of technology improved the communication between older adults, their family caregivers, and health care professionals (Åkerlind et al., 2018; Bradford et al., 2018; Quinn et al., 2019; Tseng and Hsu, 2019; Corbett et al., 2021). For instance, during an interview, a family caregiver who used the system Smarter Safer Homes shared the benefits of videoconferencing to assess the mood and state of the older adult (Bradford et al., 2018). Gutierrez et al. (2019) also showed that the Social Connector system can facilitate the interaction of family members and that video-calls were a highly appreciated activity by older adults. Tseng and Hsu (2019) found that the use of the Smart Care Interactive Systems (SCIS) with a chair significantly improved the quality of parent–child interactions. Hence, these technologies have the potential to decrease loneliness, by connecting older adults to their social network and improve the quality of relationships.
Increased sense of safety
Four studies revealed that in-home monitoring had a positive influence on feelings of safety (Cohen et al., 2016; Galambos et al., 2017; Åkerlind et al., 2018; Pais et al., 2020). For instance, older adults viewed the eHomecare system as a valuable resource to ensure safety. Family caregivers felt relief knowing that the technology was in place, because it provided information that the older adult was out of danger. It made it easier to keep balance with other responsibilities and social life (Åkerlind et al., 2018). Galambos et al. (2017) found that both family caregivers and older adults perceived an increased sense of safety using the Fall risk assessment sensor system. The Intelligent Wireless Sensor system was perceived as useful to ensure safety at home in case of falls by 34.8% of older adults and by 76.5% of family caregivers (Cohen et al., 2016). A higher proportion of older adults (74.5%) and a similar rate of family caregivers (70%) viewed the technology Domocare as useful to prevent falls and increase quality of life (Pais et al., 2020).
Reduced stress of family members and community-dwelling older adults
Improvements in communication and monitoring of potential threat is associated with stress reduction in older adults and the perception that gerontechnologies are useful to reduce family stress (Åkerlind et al., 2018; Bradford et al., 2018; Pais et al., 2020). For instance, family caregivers who used the eHomecare system noticed a decrease of concerns regarding the safety of the older adult. A total of 83% of older adults who used the Smarter Safer Homes system experienced peace of mind during the intervention (Bradford et al., 2018). Finally, older adults and family caregivers perceived that the use of Domocare could help reduce family stress by increasing the supervision of the older adult (Pais et al., 2020).
Other perceived benefits
In two studies, CDOA felt motivated to take better care of their health, after using technologies, such as the Fall Risk Assessment System (Galambos et al., 2017) and the ICMed Application (Quinn et al., 2019). Furthermore, the study on ICMed application showed that communication technologies have the potential to increase the participation of the older adult and their family caregivers in decisions regarding health (Quinn et al., 2019). Finally, the One-dose package medication support system was reported to be useful to compensate for forgetfulness and increase medication adherence (Suzuki and Hasegawa, 2018). All these benefits promote aging in place. However, several challenges need to be addressed to optimize the implementation of these technologies.
Challenges using gerontechnologies
Challenges and negative opinions have also been expressed by CDOA and their family caregivers. Their feedback is crucial for the development of gerontechnologies to be used at home that suit the profile, the preferences, and the needs of the dyads. Challenges included: (a) difficulties using the technologies, (b) technical problems, (c) privacy issues, (d) increased stress and dissatisfaction, and (d) a mismatch between values and needs.
Difficulties using the technologies
The use of technological devices often requires learning new skills. CDOA reported that learning how to correctly use technologies is a challenge (Bock et al., 2016; Bradford et al., 2018; Corbett et al., 2021). For example, older adults reported having difficulties learning how to use the technology and to identify its purpose (Bock et al., 2016). Participants reported that explaining how the data collected can be helpful to family caregivers and physicians would help them better understand their utility. It was also suggested that simplifying the visualization provided by the sensor system and demonstrations with case examples could increase its usability. In another study, older adults reported that it was challenging to adapt to a new device, especially when it served the same purpose as another technology already available in their homes (Corbett et al., 2021). Therefore, training was identified as an important need for technological implementation in older adults. Another study showed that the use of an iPad was perceived as difficult for a few older adults because of the visual and motor skills required, as well as lack of familiarity with the technology and its capabilities (Bradford et al., 2018). This is compatible with other studies with smartphones and tablet use in older adults (Barnard et al., 2013; Wilson et al., 2022).
Technical problems
Three studies reported technical problems during the intervention phase (Cohen et al., 2016; Grgurić et al., 2019; Quinn et al., 2019). First, some connectivity problems with mobile phone network occurred in rural areas while using Intelligent Wireless Sensor System (IWSS) (Cohen et al., 2016). Hence, some family caregivers did not receive the alarm messages. Connectivity issues were also found using the ICMed Application, along with log in problems (Quinn et al., 2019). Variability in the Internet connectivity caused family caregivers to receive system-offline notifications (Grgurić et al., 2019). The prolonged use of technologies like the SmartHabits system requires a change of batteries for the sensors. Battery replacement needs planning to make sure that the technology will be constantly operating at home.
Privacy issues
The perception of intrusiveness and the discomfort regarding loss of privacy is part of the downsides of environmental or personal monitoring reported by older adults (Cohen et al., 2016; Åkerlind et al., 2018; Gutierrez et al., 2019). Privacy concerns have been reported by participants in two studies (Åkerlind et al., 2018; Gutierrez et al., 2019). Feelings of being watched were experienced by older adults using the Intelligent Wireless Sensor System and triggered conflicts in some families (Cohen et al., 2016).
Increased stress and dissatisfaction
The use of gerontechnologies has a different impact on the level of stress and satisfaction. For instance, frequent false alarms can increase stress in family caregivers (Berridge et al., 2019). A few family caregivers felt annoyed by the number of alarms and calls needing to be answered (Cohen et al., 2016; Suzuki and Hasegawa, 2018). For older adults in an emergency situation, language barriers in communication while interacting with an employee of the Telecare Center can be a stressful experience for non-English speakers (Cohen et al., 2016).
Mismatch between values and needs
Studies showed that the use of technology can sometimes create a mismatch between values and needs (Suzuki and Hasegawa, 2018; Berridge et al., 2019). For instance, technologies might not match the expectation of how the older adult wished to be cared for by family members and sometimes led to conflict with family caregivers. Devices like the ODP-MSS did not allow enough flexibility in the medication administration (e.g., the older adult could not take their medication if they were away from home). As a consequence, a few older adults felt obligated to remain at home. Furthermore, four out of nine older adults perceived the technology as not useful because they could take medicine without relying on the ODP MSSS (Suzuki and Hasegawa, 2018).
Discussion
The goal of this systematic review was to summarize the research findings on in-home interventions using gerontechnologies tested simultaneously with CDOA with unimpaired cognition and their family caregivers. More specifically, we aimed to describe the technologies, their benefits and challenges, and the evidence level of the studies about them published between 2016 and 2021. We also aimed to provide recommendations for technological development, implementation, and research. To our knowledge, this is the first study synthesizing the evidence concerning the efficacy of technologies designed to support CDOA-family caregiver dyads. The review was conducted to inform older adults, family caregivers, healthcare professionals, scientists, and policymakers about the gerontechnologies available to enable them to make well-informed decisions on their use and development.
Surprisingly, we found only 13 studies meeting our eligibility criteria. The technologies were usually tested on a small sample of participants and were designed to monitor older adults, promote communication between older adults and family caregivers, help with daily tasks, and provide useful information that can be used to optimally manage their health. Most studies were conducted in the United States. Only four studies were conducted in Europe and two in Asia, even though these continents represent most of the world’s oldest population (United Nations, 2021). The majority of studies did not specify the price of the technology used, preventing people from making decisions based on the cost/efficacy. Large differences were found related to the intervention duration, ranging from 1 week (Tseng and Hsu, 2019) to 6 years (Berridge et al., 2019). The quality of studies also varied greatly, with mixed and quantitative studies receiving lower scores due to their small sample size and risk of non-response bias. Given their position in the development process, it is common for these studies to have small sample sizes. They are often the first step before conducting large implementation studies. In general, pilot studies allow for iterations to refine the technologies being tested. To our knowledge, none of these 13 studies has moved to a wider implementation phase.
Several benefits have been reported by dyads of CDOA and family caregivers, such as an increase in communication and feelings of safety. However, some gerontechnologies elicited different reactions in older adults and family caregivers, including reports of technical difficulties, learning challenges, emotional reactions (e.g., increased stress), and interpersonal difficulties (e.g., family conflicts). These differences in reaction can perhaps be addressed via co-designing technologies to facilitate their development, increase confidence levels in their use and efficacy.
The results of a systematic review of assistive technologies in dementia care showed similar results with good acceptance to facilitate daily living (Pappadà et al., 2021). Although they included intervention studies (e.g., telemedicine) and a different population (i.e., people with dementia), the potential of technology is clearly to provide monitoring and security of older adults, support in activities of daily living, and psychosocial support. The use of these technologies seems to be increasing and they can be very useful during future pandemics. Taken together, gerontechnologies provide concrete support to older adults and family caregivers when they respond to specific needs and the different problems that can be experienced in the continuum ranging from normal aging to dementia.
Currently, education about gerontechnologies and their efficacy is needed to inform the general population, clinicians, and policy-makers about the options available to promote independent living in the older adult population. Innovative solutions to quickly test, implement, and commercialize these technologies remains a challenge as there is a gap between their development and community implementation. Initiatives to educate the public in the availability of these technologies and promote research are currently underway (Aboujaoudé et al., 2023; envisAGE, https://www.envis-age.ca/en/). Still, the lack of evidence on their efficacy impedes informed decision-making. We provide the following recommendations based on the current systematic review to address some specific challenges preventing the use and dissemination of these gerontechnologies.
Recommendations for technological development, implementation, research, and public policies
Technology development
1. To develop gerontechnologies that are sensitive to the need for privacy of older adults. Privacy is an important ethical issue that must be considered during the development of gerontechnologies (Sundgren et al., 2020). For example, studies reported that cameras are less accepted because they are perceived as more intrusive (Boström et al., 2013; Claes et al., 2015). Alternative methods seem to be more appreciated by older adults (e.g., sensors for movement detection or wearable technologies for fall detection instead of cameras or microphones).
2. To develop technologies that are easy-to-use. Technologies that are easy-to-use can increase their acceptability. Also, considering potential physical, sensorial, and physical barriers in the development of gerontechnologies is a crucial step to make them more inclusive.
3. To develop technologies that respond to unmet needs at home. It is important that the functionalities respond to unmet needs identified through a co-construction process as it influences the perceived usefulness of gerontechnologies, which has been linked to positive attitudes towards their use (Chen and Chan, 2014). It is understandable that older adults would prefer using older technologies already in place instead of replacing them with new ones, since it does not require any adaptation or financial outlay.
Implementation
1. To provide training and guided practice to CDOA to help them learn new skills. Training was identified as a need in a few studies (Bock et al., 2016; Bradford et al., 2018; Corbett et al., 2021) as lack of it is a barrier to technology adoption. Training facilitates learning new skills and helps overcoming barriers to utilization of new technologies and devices (Chen and Chan, 2014). Strategies recommended include training by healthcare professionals, providing video or written instructions as well as providing access to continuous technical support. Also, providing a test period without penalty could allow older adults to explore the technologies before purchasing them to make sure that they really respond to their needs.
2. To evaluate the needs, the values, and the preferences of family caregivers and older adults simultaneously and explore the options available to the dyads. It is important that clinicians provide information about the interventions currently available and listen to the preferences of families. It is important to explore different alternatives to solve problems, such as forgetfulness, isolation, or mobility issues. Needs exploration can help families make informed choices and increase their feeling of self-determination, which is important to promote psychosocial health (Ntoumanis et al., 2021). Also, personalizing the interventions can ensure optimal results in CDOA and their family caregivers in their unique social, economic, and environmental context (Ebrahimi et al., 2021).
3. To ensure that the intervention proposed matches the current physical and cognitive autonomy level of the older adult. It has been found that interventions are perceived as more acceptable depending on the perception of the benefits of the technology. For instance, older adults are more likely to accept monitoring technology when experiencing mobility issues if it allows them to stay in their homes. In contrast, feelings of being able to perform a daily activity without the technology can lead older adults to perceive it as not useful (Tseng and Hsu, 2019). More importantly, it can have negative consequences on older adults, such as increasing their feeling of becoming dependent on the technology to do something that they can still do without it.
Research
1. To adopt a co-construction approach. To maximize the agency of older adults and their family caregivers and to ensure that the interventions match their values and needs, we encourage the active consultation and participation of community stakeholders in research on development and adaptation of gerontechnologies (Closon and Léonard, 2016). Researchers are encouraged to describe the phases of development of their technologies, including the co-construction process and the persons involved in the different iterations.
2. To document the effects of interventions on quality of life, well-being and other psychological outcomes in CDOA and their family caregivers. In the majority of the studies included in this systematic review, these effects were not documented and would provide additional evidence of the benefits of gerontechnologies for the dyads of CDOA and their family caregivers. Personal variables are important in technology adoption.
3. To conduct scaled evaluation and implementation. Future studies must evaluate the effectiveness of interventions using gerontechnology with end-users and clinicians, in real-world contexts (e.g., integration in current psychosocial or nursing interventions). These studies should include different contexts to generate evidence of generalizability (e.g., different populations of older adults and geographical locations). Conducting randomized control trials with bigger samples of CDOA and family caregivers is not always possible considering the costs both of the technological development itself and of the research. However, alternative research methods can be used. For instance, interrupted time series or single pretest-post designs can be used (Wang et al., 2021)
Public policies
1. To give access to information and training on gerontechnologies to managers and healthcare professionals. This step is important to facilitate implementation of gerontechnologies for home support in different organizations (e.g., the healthcare system). University curricula need to include more training in technology, rehabilitation, and older adults’ needs.
2. To fund studies evaluating the cost-effectiveness of interventions using gerontechnologies. This recommendation is based on the absence of studies evaluating the cost-effectiveness of interventions using gerontechnologies for CDOA and family caregivers. This type of study is crucial to influence future governmental investments for home support.
General conclusion
This systematic review identified gerontechnologies that have been tested to support aging in place among among CDOA without cognitive impairment and their family caregivers. It provided information on the benefits and challenges perceived by the dyads, the quality level of the studies included, and some recommendations to address challenges linked to dissemination and implementation of these technologies.
Gerontechnologies are an innovative solution to help older adults age in place and maintain their autonomy and independence. Efforts must be made by scientists, healthcare professionals, and policy-makers to make these interventions accessible and adapted to the specific challenges encountered by older adults and their families.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
The Ministère de l’Économie, de l’Innovation et de l’Énergie (MEIE Grant number 21-24-PSOv2a-53186) du Québec provided scholarships to support the students participating in this article (M-CS, HS, HD, CC, and KA). AGE-WELL and the Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, CIUSSS du Centre-Sud-de-l’Île-de-Montréal provided a Graduate Student Award in Technology and Aging to support one of the graduate students participating in the project (HS).
Acknowledgments
The authors would like to thank Marc-Olivier Croteau, M. Sc., M.S.I. (Librarian at Université de Montréal) and Audrey Attia, M.S.I. (Librarian at the Geriatrics and Gerontology Library of the Centre de recherche de l’Institut universitaire de gériatrie de Montréal – CRIUGM) who helped to refine and perform the search strategy for this systematic review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aboujaoudé, A., Filiou, R.-P., Belchior, P., Couture, M., and Bier, N.. Inventory of technologies to support aging in place (2023) Technology to support aging in place: An inventory of technologies available in Quebec [Digital Inventory]. Retrieved from Centre de recherche de l’Institut universitaire de gériatrie de Montréal website : https://criugm.qc.ca/en/research/inventory-of-technologies-to-support-aging-in-place/
Åkerlind, C., Martin, L., and Gustafsson, C. (2018). eHomecare and safety: the experiences of older patients and their relatives. Geriatric Nurs 39, 178–185. doi: 10.1016/j.gerinurse.2017.08.004
Alves, L. C. D. S., Monteiro, D. Q., Bento, S. R., Hayashi, V. D., Pelegrini, L. N. C., and Vale, F. A. C. (2019). Burnout syndrome in informal caregivers of older adults with dementia: a systematic review. Dement. Neuropsychol. 13, 415–421. doi: 10.1590/1980-57642018dn13-040008
Barnard, Y., Bradley, M. D., Hodgson, F., and Lloyd, A. D. (2013). Learning to use new technologies by older adults: Perceived difficulties, experimentation behaviour and usability. Computers in Human Behavior, 29, 1715–1724. doi: 10.1016/j.chb.2013.02.006
Berridge, C., Chan, K. T., and Choi, Y. (2019). Sensor-based passive remote monitoring and discordant values: qualitative study of the experiences of low-income immigrant elders in the United States. JMIR Mhealth Uhealth 7:e11516. doi: 10.2196/11516
Bock, C., Demiris, G., Choi, Y., le, T., Thompson, H. J., Samuel, A., et al. (2016). Engaging older adults in the visualization of sensor data facilitated by an open platform for connected devices. Technol Health Care 24, 541–550. doi: 10.3233/THC-161150
Boström, M., Kjellström, S., and Björklund, A. (2013). Older persons have ambivalent feelings about the use of monitoring technologies. Technol. Disabil. 25, 117–125. doi: 10.3233/tad-130376
Bradford, D. K., Kasteren, Y. V., Zhang, Q., and Karunanithi, M. (2018). Watching over me: positive, negative and neutral perceptions of in-home monitoring held by independent-living older residents in an Australian pilot study. Ageing Soc. 38, 1377–1398. doi: 10.1017/s0144686x1700006x
Chen, K., and Chan, A. H. S. (2014). Gerontechnology acceptance by elderly Hong Kong Chinese: a senior technology acceptance model (STAM). Ergonomics 57, 635–652. doi: 10.1080/00140139.2014.895855
Claes, V., Devriendt, E., Tournoy, J., and Milisen, K. (2015). Attitudes and perceptions of adults of 60 years and older towards in-home monitoring of the activities of daily living with contactless sensors: an explorative study. Int. J. Nurs. Stud. 52, 134–148. doi: 10.1016/j.ijnurstu.2014.05.010
Closon, M. C., and Léonard, M. C. (2016). Chapitre 3. Favoriser concrètement le rôle actif et citoyen de la personne âgée: une application du care capacitant. J. Int. Bioethique 27, 53–68. doi: 10.3917/jib.273.0053
Colnar, S., Dimovski, V., Grah, B., Rogelj, V., and Bogatajow, D.. (2020) Gerontechnology: literature review and research agenda, In 2020 59th Annual Conference of the Society of Instrument and Control Engineers of Japan (SICE). 391–396. IEEE. doi: 10.23919/SICE48898.2020.9240225
Corbett, C., Combs, E., Wright, P., Owens, O., Stringfellow, I., Nguyen, T., et al. (2021). Virtual home assistant use and perceptions of usefulness by older adults and support person dyads. Int. J. Environ. Res. Public Health 18:1113. doi: 10.3390/ijerph18031113
Crichton, M., Craven, D., Mackay, H., Marx, W., de van der Schueren, M., and Marshall, S. (2019). A systematic review, meta-analysis and meta-regression of the prevalence of protein-energy malnutrition: associations with geographical region and sex. Age Ageing 48, 38–48. doi: 10.1093/ageing/afy144
Cohen, C., Kampel, T., and Verloo, H. (2016). Acceptability of an intelligent wireless sensor system for the rapid detection of health issues: Findings among home-dwelling older adults and their informal caregivers. Patient Preference and Adherence, 10, 1687–1695. doi: 10.2147/PPA.S113805
Di Lorito, C., Masud, T., Gladman, J., Godfrey, M., Dunlop, M., Bosco, A., et al. (2021). Deconditioning in people living with dementia during the COVID-19 pandemic: Qualitative study from the promoting activity, independence and stability in early dementia (praised) process evaluation. BMC Geriatrics, 21, 1–10. doi: 10.1186/s12877-021-02451-z
Ebrahimi, Z., Patel, H., Wijk, H., Ekman, I., and Olaya-Contreras, P. (2021). A systematic review on implementation of person-centered care interventions for older people in out-of-hospital settings. Geriatric Nurs 42, 213–224. doi: 10.1016/j.gerinurse.2020.08.004
Fakoya, O. A., McCorry, N. K., and Donnelly, M. (2020). Loneliness and social isolation interventions for older adults: a scoping review of reviews. BMC Public Health 20:129. doi: 10.1186/s12889-020-8251-6
Galambos, C., Rantz, M., Back, J., Jun, J. S., Skubic, M., and Miller, S. J. (2017). Older adults’ perceptions of and preferences for a fall risk assessment system: exploring stages of acceptance model. Comput Inform Nurs 35, 331–337. doi: 10.1097/CIN.0000000000000330
Grgurić, A., Mošmondor, M., and Huljenić, D. (2019). The SmartHabits: an intelligent privacy-aware home care assistance system. Sensors 19:907. doi: 10.3390/s19040907
Gutierrez, F. J., Muñoz, D., Ochoa, S. F., and Tapia, J. M. (2019). Assembling mass-market technology for the sake of wellbeing: a case study on the adoption of ambient intelligent systems by older adults living at home. J. Ambient. Intell. Humaniz. Comput. 10, 2213–2233. doi: 10.1007/s12652-017-0591-4
Halicka, K. (2019). Gerontechnology-the assessment of one selected technology improving the quality of life of older adults. Engin Manage Product Serv 11, 43–51. doi: 10.2478/emj-2019-0010
Hong, Q. N., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., et al. (2018). The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 34, 285–291. doi: 10.3233/efi-180221
Hurstfield, J., Parashar, U., and Schofield, K. (2007). The costs and benefits of independent living. Office Disabil. Issues. Available at: https://sid-inico.usal.es/idocs/F8/FDO19730/independent_living_report.pdf (Accessed: January 5, 2024).
Ikeda, Y., Maruta, M., Shimokihara, S., Nakamura, A., Han, G., and Tabira, T. (2021). Difficulties in the use of everyday technology among older adults with subjective memory complaint and cognitive decline. Gerontology 68, 655–663. doi: 10.1159/000518390
Kim, J. (2021). Housing accessibility for seniors with mobility and grasping disabilities: lessons from the American housing survey. Hous. Stud. 36, 758–783. doi: 10.1080/02673037.2020.1729963
Leslie, M., Gray, R. P., and Khayatzadeh-Mahani, A. (2021). What is 'care quality' and can it be improved by information and communication technology? A typology of family caregivers' perspectives. Scand. J. Caring Sci. 35, 220–232. doi: 10.1111/scs.12837
Liao, X., Wang, J., Zhang, F., Luo, Z., Zeng, Y., and Wang, G. (2022). The levels and related factors of compassion fatigue and compassion satisfaction among family caregivers: a systematic review and meta-analysis of observational studies. Geriatric Nurs 45, 1–8. doi: 10.1016/j.gerinurse.2022.02.016
Moreland, B., Kakara, R., and Henry, A. (2012). Trends in nonfatal falls and fall-related injuries among adults aged ≥65 years-United States. Morb. Mortal. Wkly Rep. 69, 875–881. doi: 10.15585/mmwr.mm6927a5
Ntoumanis, N., Ng, J. Y. Y., Prestwich, A., Quested, E., Hancox, J. E., Thøgersen-Ntoumani, C., et al. (2021). A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 15, 214–244. doi: 10.1080/17437199.2020.1718529
Pais, B., Buluschek, P., DuPasquier, G., Nef, T., Schütz, N., Saner, H., et al. (2020). Evaluation of 1-year in-home monitoring technology by home-dwelling older adults, family caregivers, and nurses. Front. Public Health 8:518957. doi: 10.3389/fpubh.2020.518957
Pappadà, A., Chattat, R., Chirico, I., Valente, M., and Ottoboni, G. (2021). Assistive technologies in dementia care: an updated analysis of the literature. Front. Psychol. 12:644587. doi: 10.3389/fpsyg.2021.644587
Quinn, C. C., Staub, S., Barr, E., and Gruber-Baldini, A. (2019). Mobile support for older adults and their caregivers: dyad usability study. JMIR Aging 2:e12276. doi: 10.2196/12276
StatCan Recours aux soins à domicile et besoins non satisfaits en matière de soins à domicile au Canada, 2021 (2022) Available at: Statcan.gc.ca and https://www.150.statcan.gc.ca/n1/daily-quotidien/220826/dq220826a-fra.htm (Accessed: May 29, 2023).
Sundgren, S., Stolt, M., and Suhonen, R. (2020). Ethical issues related to the use of gerontechnology in older people care: a scoping review. Nurs. Ethics 27, 88–103. doi: 10.1177/0969733019845132
Suzuki, R., and Hasegawa, T. (2018). Evaluation of a one-dose package medication support system for community-based elderly patients and eldercare facilities. Am. J. Health System Pharm. 75, e202–e212. doi: 10.2146/ajhp170176
Tseng, W. S.-W., and Hsu, C.-W. (2019). A smart, caring, interactive chair designed for improving emotional support and parent-child interactions to promote sustainable relationships between elderly and other family members. Sustainability 11:961. doi: 10.3390/su11040961
United Nations: (2021) Department of Economic and Social Affairs: Population Division. World population ageing 2019. New York, NY: United Nations.
Veritas Health Innovation. (2014). Covidence systematic review software. Available at: https://www.covidence.org/
Wang, R. H., Kenyon, L. K., McGilton, K. S., Miller, W. C., Hovanec, N., Boger, J., et al. (2021). The time is now: a FASTER approach to generate research evidence for technology-based interventions in the field of disability and rehabilitation. Arch. Phys. Med. Rehabil. 102, 1848–1859. doi: 10.1016/j.apmr.2021.04.009
Keywords: Gerontechnology, AgeTech, Community-Dwelling Older Adults (CDOA), Family Caregivers (FC), Aging in place, Home support, Older adult, Aging
Citation: Moreno A, Scola M-C, Sun H, Durce H, Couve C, Acevedo K and Gutman GM (2024) A systematic review of gerontechnologies to support aging in place among community-dwelling older adults and their family caregivers. Front. Psychol. 14:1237694. doi: 10.3389/fpsyg.2023.1237694
Edited by:
Rüdiger Christoph Pryss, Julius Maximilian University of Würzburg, GermanyReviewed by:
Alvaro Garcia Soler, Matia Gerontological Institute, SpainXichenhui Qiu, Shenzhen University, China
Copyright © 2024 Moreno, Scola, Sun, Durce, Couve, Acevedo and Gutman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexander Moreno, jhon.alexander.moreno.1@umontreal.ca
†These authors share first authorship